Introduction
Spitz nevus, first described by Sophie Spitz in 1948, is a benign melanocytic neoplasm commonly seen in young individuals, particularly females1. Clinically, it can mimic various conditions, including melanoma, basal cell carcinoma, and dermatofibroma, making histopathological examination essential for accurate diagnosis2. Although typically benign, complete surgical excision is often recommended due to its difficulty in differentiating it from malignant melanocytic lesions3.
Case report
A 22-year-old female presented to the dermatology outpatient department with a solitary lesion on her left cheek, which had been present for 4 years. The lesion developed insidiously without any preceding history of trauma, insect bites, or inflammation. The patient had no significant personal or family history of skin disorders. She sought medical attention due to cosmetic concerns.
On dermatological examination, the lesion was a well-circumscribed, firm, dome-shaped, oval nodule measuring approximately 1.0 cm × 1.5 cm (Fig. 1). The lesion had a slightly pink hue with mild hyperpigmentation in the centre. The surface was smooth without ulceration, scaling, or crusting. The lesion was not fixed to the underlying structures, and there was no regional lymphadenopathy. Sensory and motor examinations were unremarkable.

Figure 1. A well-circumscribed dome-shaped nodule on the left side of the face.
Based on the clinical presentation, the differential diagnoses included intradermal nevus, desmoplastic nevus, melanoma, basal cell carcinoma, dermatofibroma, pseudolymphoma, and histoid leprosy.
The lesion was completely excised with primary closure. The excised tissue was sent for histopathological evaluation. Hematoxylin and eosin staining revealed a well-circumscribed dermal lesion composed of large spindle-shaped melanocytic cells arranged in nests (Fig. 2). The nevus cells were symmetrically placed with well-defined clefts between the junctional nests and the surrounding epidermis (Fig. 3). There was mild pigment incontinence, but no cellular atypia or mitotic figures were observed. These findings were consistent with a diagnosis of Spitz nevus.
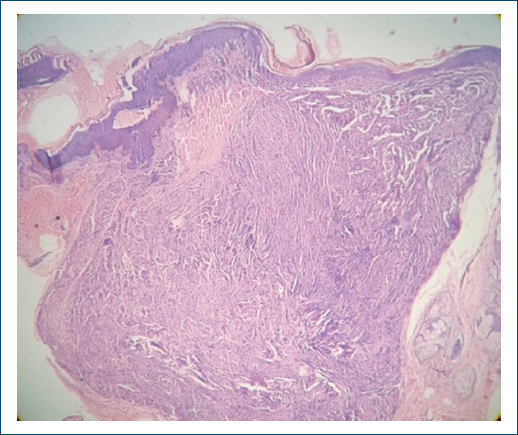
Figure 2. H&E stain (×10 magnification) showing well-circumscribed junctional and dermal nest of spindled-shaped melanocytic cells.
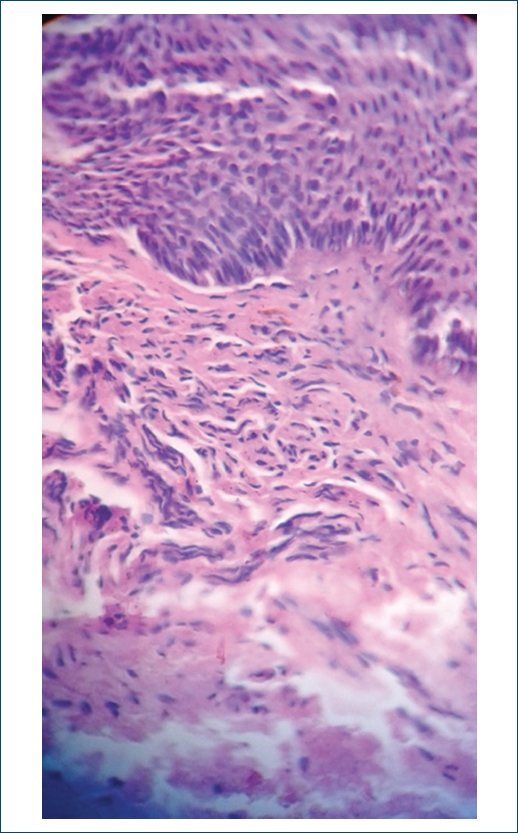
Figure 3. H&E stain (×40 magnification) showing clefts in between the nests of spindle-shaped nevus cells.
Discussion
Spitz nevus is a benign melanocytic proliferation that primarily occurs in children and young adults1. It is characterized by the spindle and epithelioid melanocytes arranged in nests within the dermis or at the dermo-epidermal junction3. Clinically, it can be confused with malignant melanocytic lesions, necessitating histopathological confirmation2.
Spitz nevus can exhibit a range of histopathological patterns, including conventional (classic), desmoplastic, pigmented, and angiomatoid subtypes4. The presence of clefts separating the nevus cells from the epidermis and a well-circumscribed symmetrical arrangement are distinguishing features4. Unlike malignant melanomas, Spitz nevi typically lack significant cellular atypia and mitotic activity5.
While Spitz nevus is generally considered benign, rare cases of atypical Spitz tumors with uncertain malignant potential have been reported, necessitating long-term follow-up in select cases3. Recent studies suggest that immunohistochemical markers such as p16, Ki-67, and HMB-45 can aid in distinguishing Spitz nevi from malignant melanomas6. In addition, molecular techniques, such as FISH and CGH are proving useful in differentiating atypical Spitz tumors from other melanocytic proliferations7. The use of molecular markers, such as HRAS mutations and gene fusions, has been identified in Spitz nevi, offering a new avenue for diagnostic refinement7.
The standard treatment for Spitz nevus is complete surgical excision, both for diagnostic purposes and to prevent misdiagnosis8.
Conclusion
This case highlights the importance of considering Spitz nevus in the differential diagnosis of solitary pigmented nodules, especially in young individuals. Given its potential for clinical confusion with malignant lesions, histopathological and molecular confirmations remain the gold standard for diagnosis. Complete surgical excision is the preferred management approach for both diagnostic accuracy and cosmetic concerns. The incorporation of molecular and immunohistochemical techniques can enhance diagnostic precision and improve patient management.
Funding
None.
Conflicts of interest
None.
Ethical considerations
Protection of human subjects and animals. The authors declare that no experiments on humans or animals were performed for this research.
Confidentiality, informed consent, and ethical approval. The authors have followed their institution’s confidentiality protocols, obtained informed consent from all patients, and secured approval from the Ethics Committee. SAGER guidelines have been followed as applicable to the nature of the study.
Declaration on the use of artificial intelligence (AI). The authors declare that no generative artificial intelligence was used in the writing or creation of the content of this manuscript.
