Introduction
Lupus erythematosus is an autoimmune disease that commonly affects the skin. It encompasses a spectrum of different cutaneous manifestations, among which discoid lupus erythematosus (DLE) is one of the most common among chronic forms. DLE often manifests as scaly, erythematous plaques with potential permanent scarring and pigmentary changes, significantly impacting patients’ quality of life. It predominantly affects photoexposed sites, such as the face and scalp, although lesions may occur in other locations. DLE may signal systemic lupus erythematosus (SLE) in a subset of cases, particularly in the generalized form. Treatment of DLE may prove difficult, and delaying effective treatment can lead to permanent scarring and disfiguration.
Case report
A 53-year-old Caucasian female patient, smoker, with no other relevant medical history was referred to the Dermatology Clinic with a 1-year history of alopecia and erythematous lesions on the face.
On physical examination, an extensive erythematous infiltrated plaque of cicatricial alopecia was observed across almost the entire sagittal region, with peripheral hyperpigmentation. The patient also presented two well-defined erythematous plaques, on the left malar and glabellar region, with central scaling and peripheral hyperpigmentation.
The patient had no other complaints and an unremarkable complete blood count and biochemical panel, as well as an antinuclear antibodies test of 1:80, negative anti-double-stranded DNA antibody, and serum complement levels (C3 and C4) within the reference range, making the presence of systemic disease unlikely.
A 6 mm punch skin biopsy was performed on the scalp, showing areas of follicular keratosis in the epidermis, with vacuolar degeneration in the basal layer and acidophilic bodies. There was a dermal perivascular and periadnexial lymphohistiocytic infiltrate (Figs. 1 and 2). These findings were consistent with the clinical diagnosis of discoid cutaneous lupus erythematosus.
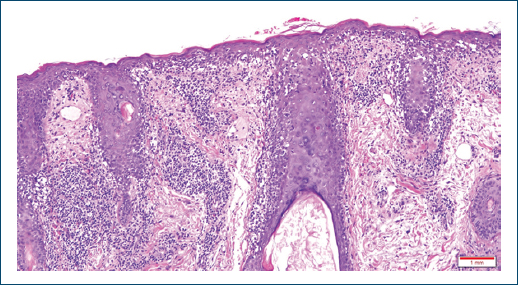
Figure 1. (H&E ×40) Epidermis with follicular keratosis and areas of vacuolar degeneration of the basal layer. In the dermis, a superficial and deep perivascular lymphohistiocytic and periadnexal inflammatory infiltrate is observed. There is also vascular dilation and foci of interstitial hemorrhage.
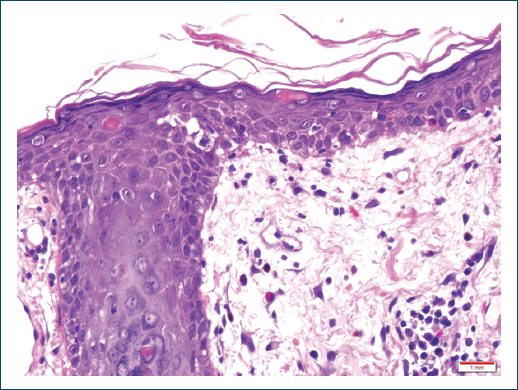
Figure 2. (H&E ×400) Higher amplification, showcasing follicular keratosis, vacuolar degeneration of the basal layer, and the presence of acidophilic bodies.
The patient was initially treated with topical betamethasone and strict photoprotection, with no improvement and even with the appearance of new lesions on the face, trunk, and upper limbs. Given the widespread nature of lesions, intralesional corticosteroid therapy was not proposed, and the patient was started on hydroxychloroquine 400 mg daily and a course of oral prednisolone, with transient improvement but worsening during tapering. At this point, oral methotrexate was added and titrated up to 15 mg weekly, with subsequent discontinuation due to moderate gastrointestinal intolerance and lack of response. Therapeutic trials with acitretin 10 mg daily and dapsone, titrated to 100 mg daily, were also conducted, but both were unsuccessful, with an increase in lesion size. We later started treatment with mycophenolate mofetil (MMF), titrated up to 2 g/day, which finally allowed control of the disease, with improvement of inflammatory signs of the lesions and stabilization of their size. Complete blood count, liver enzymes, and renal function were assessed 2 weeks after treatment initiation and subsequently repeated every other month, with progressive spacing of follow-up laboratory evaluations. No new lesions developed after the patient was started on MMF and there was very significant clinical improvement after 10 months of therapy with MMF in several locations (Figs. 3–10). The treatment was well tolerated, with no reported side effects. The patient maintains follow-up and remains without disease activity 15 months after initiating treatment.
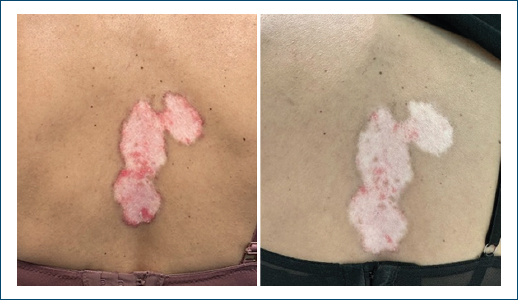
Figure 3. Lesions of discoid lupus erythematosus on the back before (left) and after (right) 10 months of therapy with mycophenolate mofetil.
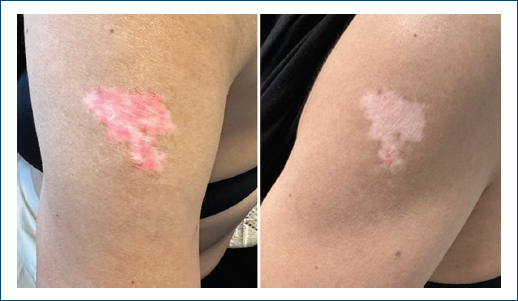
Figure 4. Lesions of discoid lupus erythematosus on the left arm before (left) and after (right) 10 months of therapy with mycophenolate mofetil.

Figure 5. Right retroauricular lesions of discoid lupus erythematosus before (left) and after (right) 10 months of therapy with mycophenolate mofetil.
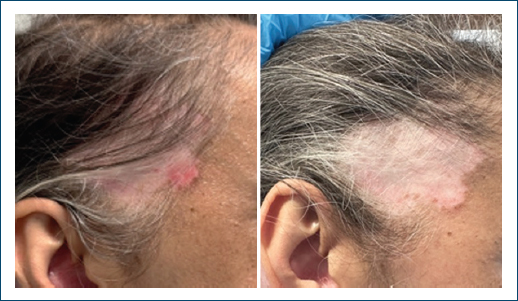
Figure 6. Right frontotemporal lesions of discoid lupus erythematosus before (left) and after (right) 10 months of therapy with mycophenolate mofetil.

Figure 7. Left facial and retroauricular lesions of discoid lupus erythematosus before (left) and after (right) 10 months of therapy with mycophenolate mofetil.

Figure 8. Right mandibular lesions of discoid lupus erythematosus before (left) and after (right) 10 months of therapy with mycophenolate mofetil.

Figure 9. Presternal lesion of discoid lupus erythematosus before (left) and after (right) 10 months of therapy with mycophenolate mofetil.
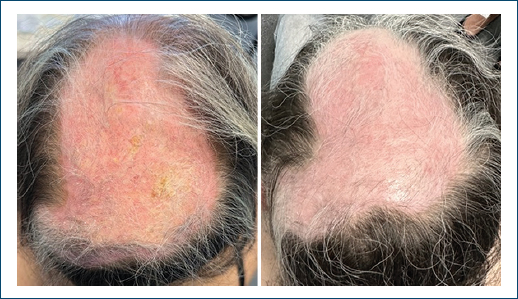
Figure 10. Scalp lesion of discoid lupus erythematosus before (left) and after (right) 10 months of therapy with mycophenolate mofetil.
Discussion
To date, there are no well-established therapeutic guidelines for cutaneous lupus refractory to first-line drugs, including DLE. Fortunately, most patients respond to treatment with topical/intralesional corticosteroids, topical calcineurin inhibitors, oral anti-malarial drugs, and photoprotection. The generalized forms of DLE increase the risk of SLE and may prove more difficult to treat.
MMF is an immunosuppressant drug that is generally well tolerated and reversibly inhibits the enzyme inosine monophosphate dehydrogenase (involved in the synthesis of purines). Diarrhea, vomiting, nausea, and low cellular blood count levels are the most common side effects1.
There is limited evidence of the benefit of MMF in cutaneous lupus, including DLE, consisting only of retrospective studies and case reports. Furthermore, most studies tend to include in their cohort patients with several subtypes of cutaneous lupus. Even though most treatment recommendations assemble several forms of cutaneous lupus, it is not certain that all disease subtypes share the same response to a given treatment.
We reviewed all publications available at the MEDLINE database regarding the use of MMF in DLE, excluding papers that included exclusively other forms of cutaneous lupus and focusing on the results of the subset of patients diagnosed with DLE. A 2021 retrospective study from Keyes et al. showed similar results in patients with discoid or subacute cutaneous lupus treated with either methotrexate or MMF. However, their results showed a trend favoring treatment with MMF in the 40 patients with DLE, albeit with no statistical significance2. In another retrospective study from 2019, including patients with both subacute and discoid lupus, Gammon B. and colleagues found some improvement after MMF treatment in all 19 subjects with DLE. Regarding these 19 cases, eight patients showed a complete response to treatment, defined as complete or near-complete resolution of disease activity; eight patients had a partial response; and three patients had complete responses followed by flares of the disease3. Contradictorily, a former retrospective study from 2005, including three patients with DLE treated with MMF, concluded that the drug was ineffective in these patients, highlighting one case of disease flare after starting the drug4.
The remaining evidence consists only of case series and case reports, accounting for a total of five cases with complete or near-complete responses to treatment with MMF – three patients with a palmoplantar variant of DLE5,6, one case of lupus profundus7, and one case of DLE associated with chilblain lupus7. Bardazzi et al. refer that MMF may be an effective treatment option in patients with palmoplantar disease; a rare variant that commonly has a poor response to treatment5.
This case aims to illustrate the difficulty of treating refractory DLE and supports a potential role of MMF in refractory disease. The literature review showed a lack of substantial evidence for the use of MMF in DLE, and the comprehension of the role of this drug is further aggravated by the fact that most studies include only patients with disease refractory to the most common treatment modalities (including topical therapies, hydroxychloroquine, and methotrexate) and, in some case, other second and third line options. This bias is emphasized by most of the cited authors. As mentioned previously, the inclusion of all subtypes of cutaneous lupus may act as a confounding factor. Keyes et al. hint at a possible difference in response to MMF among patients with DLE, compared to patients with subacute cutaneous lupus erythematosus2. Further studies, ideally randomized trials, are needed to clarify the role of this drug in DLE and other forms of cutaneous lupus.
Conclusion
This case highlights the therapeutic challenge posed by refractory discoid lupus erythematosus and illustrates the potential effectiveness and tolerability of mycophenolate mofetil in achieving sustained disease control after failure of multiple conventional therapies. Although current evidence remains limited to retrospective studies and case reports, our findings add to the growing body of literature suggesting a role for mycophenolate mofetil in selected patients with severe or treatment-resistant DLE. Well-designed prospective studies are needed to better define its efficacy, optimal positioning, and long-term safety in this patient population.
Funding
None.
Conflicts of interest
None.
Ethical considerations
Protection of human subjects and animals. The authors declare that no experiments on humans or animals were performed for this research.
Confidentiality, informed consent, and ethical approval. The authors have followed their institution’s confidentiality protocols, obtained informed consent from all patients, and secured approval from the Ethics Committee. SAGER guidelines have been followed as applicable to the nature of the study.
Declaration on the use of artificial intelligence (AI). The authors declare that no generative artificial intelligence was used in the writing or creation of the content of this manuscript.
