Introduction
Melanoma is one of the types of malignant neoplasms that present the fastest growing incidence rate. Despite representings < 5% of all malignant skin neoplasms, it is globally responsible for the majority of deaths due to skin cancer1.
In 2022, the occurrence of 331,000 cases of melanoma and about 57,000 deaths worldwide was estimated2. The highest incidence rates per 100,000 inhabitants were observed in Australia and New Zealand (42 in men and 31 in women), in Western Europe (19 in men and in women), in North America (18 in men and 14 in women), and in Northern Europe (17 in men and 18 in women)3.
Incidence has been increasing over the past 50 years. In the United States, the probability of being diagnosed with invasive cutaneous melanoma increased from 1 in 1,500 in 1930 to 1 in 34 in 20154. Estimates further indicate that 500,000 new cases of melanoma per year and 100,000 deaths are expected by 2040. This increase in incidence highlights the urgency of implementing specific and effective measures for melanoma prevention3.
The main risk factors associated with melanoma are exposure to ultraviolet (UV) radiation, a history of sunburns (particularly in childhood), skin phototype (fair skin, red or blond hair, blue eyes), and personal or family history of melanoma. However, exposure to UV radiation, from sunlight or artificial sources, is described as the main environmental risk factor, associated with about 70% of cutaneous melanoma cases5.
Melanoma is considered a highly preventable type of cancer. Primary and secondary prevention strategies can reduce incidence and potentially lower mortality. Primary prevention mainly consists of avoiding risk factors and adopting effective sun protection habits, while secondary prevention consists of early detection.
Avoiding both sun exposure and artificial tanning, and using protective clothing are also recommended photoprotection strategies, associated with a decreased risk of developing the disease.
The use of sunscreen is described as one of the fundamental strategies in primary prevention. It is estimated that it can reduce its incidence and the occurrence of invasive melanomas6 and that its daily use is cost-effective and should be a priority in prevention7.
Educational campaigns also play a fundamental role in raising public awareness about the risks of sun exposure and are tools for promoting effective sun protection behaviors and habits. However, it is important that these are adapted to the population’s knowledge and beliefs so that motivation increases and leads to improvements in preventive behaviors.
Several studies also assess how technology, personalized risk assessment tools, and interventions tailored to risk profile can influence behavior change and, consequently, reduce or not the incidence of melanoma.
Although primary prevention strategies are today considerably recommended and studies support their effectiveness in melanoma prevention, historically some inconsistencies regarding their effectiveness8 have been found9. For example, evidence regarding sunscreen use was quite inconsistent, although today it is considered an effective, safe6, and cost-effective10 measure.
Particularly at the level of primary health care, there is evidence regarding the effectiveness of behavioral counseling, population education, and awareness campaigns. However, there is still discussion about which theoretical approaches are most appropriate, what the ideal intensity and duration of counseling should be, and regarding appearance-based interventions (ABi) (photoaging) compared to health-based interventions (HBi)11.
Prevention measures involving genetic risk assessment and the provision of personalized information according to individual risk are also controversial. While several studies report that personalized interventions are more effective than generic ones, others do not appear to find greater effectiveness12.
The effectiveness of using technology, such as digital interventions, mobile applications, and direct-to-consumer genetic testing in primary prevention, is also questionable9. Although technology is very promising in melanoma prevention, evidence on benefits and cost-effectiveness is still limited.
Thus, this work aims, through a literature review, to gather information about primary prevention strategies for melanoma, through an analysis of the most recent findings, inconsistencies, and limitations of 21st-century literature. It, therefore, seeks a better understanding of the effectiveness of different strategies, to identify priorities for future studies, and ultimately to optimize prevention strategies to reduce the incidence of melanoma.
Methodology
This study was conducted as a systematic review of the literature in accordance with Preferred Reporting Items for Systematic reviews and Meta-Analyses guidelines. The diagram in figure 113 presents the article selection process.
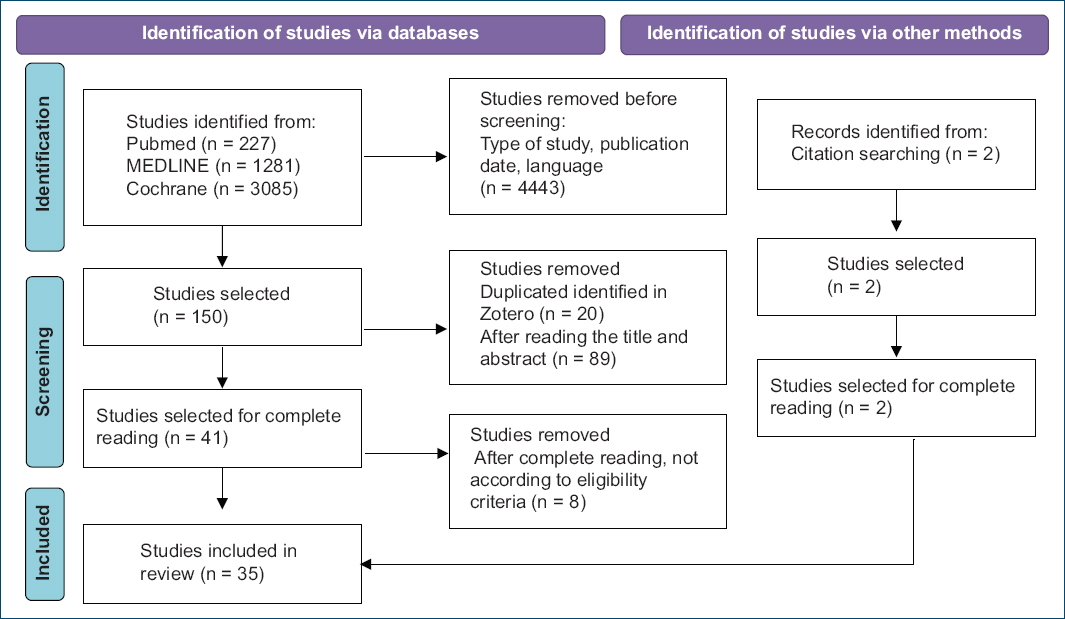
Figure 1. Preferred Reporting Items for Systematic reviews and Meta-Analyses flow diagram (adapted from Page MJ, et al. BMJ 2021;372:n71.doi: 10.1136/bmj.n71)13.
Search strategy and eligibility criteria
The PICO method was used to define the sample and the inclusion and exclusion criteria of the articles, which are presented in table 1.
Table 1. Eligibility criteria
| Inclusion criteria | Population aged 18 years or olderInclusion of primary prevention strategiesPublications from January 2000 to November 30, 2025Articles in English, Portuguese, or SpanishInclusion of melanomaFree articles or articles accessible through the Faculty of Medicine of the University of Lisbon |
| Exclusion criteria | Population under 18 years of ageNo inclusion of primary prevention strategiesPublications before the year 2000Articles in languages not included in the inclusion criteria (Portuguese, English, or Spanish)Exclusion of melanomaPaid articles or articles not accessible through the Faculty of Medicine of the University of Lisbon |
- P. Participants: adults aged 18 years or older.
- I. Intervention: primary prevention strategies.
- C. Comparison: other primary prevention strategies, no prevention strategy, secondary prevention strategies.
- O. Outcome: incidence of melanoma/melanoma mortality/effectiveness of the applied strategy/frequency of sunburns/photoprotection behaviors.
A comprehensive literature search was performed in the following databases: PubMed, MEDLINE, and the Cochrane Library. The search was conducted between November 2024 and January 2025. The search strategy was developed iteratively and combined controlled vocabulary terms and free-text keywords related to melanoma and primary prevention. Core search terms were combined using Boolean operators and the final search strategy was adapted for each database. The search carried out with Boolean operators through a single line approach, improved multiple times over time. The first search in November 2024 yielded 227 results in PubMed, 1,281 in MEDLINE, and 3,085 in Cochrane (Supplementary Table 1).
At the end of January 2025, after the different tests of the search strategy and changes in keywords, the results were limited to a total of 150 (54 results in PubMed, 10 in MEDLINE, and 86 in Cochrane) shown above. All the 150 articles were added to an Excel table reproduced in supplementary table 3, titles and abstracts of all articles were read, with identification of inclusion or exclusion criteria for eligibility.
Of the 150 articles, 61 were selected after screening of title and abstract (“eligibile” on Supplementary Table 3). The 61 articles were then added to the reference manager Zotero and, using this software, 20 duplicates were removed. After this, the 41 articles left were read in full. Of these 41 articles, 33 were selected as they fully met the eligibility criteria. An additional two articles were later found based on citation reading and included. In total, 35 articles were included in the systematic review.
The complete search strategy and procedure for all databases are detailed in the supplementary data.
Risk of bias assessment
Studies were evaluated for inclusion based on the predefined eligibility criteria. Each study was reviewed and decisions regarding inclusion were made based on these criteria. No independent formal risk-of-bias assessment was conducted.
Results
At the end 35 articles were included in the systematic review, with information regarding study type, participants, intervention and comparison, results, conclusions, limitations, and topic/primary prevention strategy presented in supplementary data.
The general themes/primary prevention strategies were divided into the following thematic codes:
- – BC: behavioral counseling, education, and population awareness
- – T: technology, mobile applications, online interventions, multimedia resources, and/or message sending
- – G: genetic information, personalized risk information
- – CQ: chemoprotective agents.
Discussion
From the studies included, eight focus on strategies of behavioral counseling, education, and population awareness (BC). Fourteen combined these approaches with the use of technology, online interventions, mobile applications, and/or message sending (T). Ten studies integrated behavioral counseling with the use of genetic information or personalized information on the individual risk (G). Three studies addressed the use of chemoprotective agents (CQ).
Behavioral counseling, education, and population awareness (BC)
Among primary melanoma prevention strategies, measures such as the use of sunscreen, protective clothing, seeking shade, and avoiding sun exposure during peak hours stand out across studies.
The use of sunscreen is consistently highlighted as an effective and accessible measure. Green et al. demonstrated that the regular use of sunscreen with a sun protection factor equal to or > 15 could be associated with up to a 73% reduction in the risk of developing invasive melanoma, and suggests that melanoma is, to a large extent, preventable through the regular use of sunscreen6.
Hirst et al. and Gordon et al. concluded that the systematic use of sunscreen could prevent a significant number of new skin cancer cases and substantially contribute to the reduction of health care costs over up to 30 years. Therefore, primary prevention based on the daily use of sunscreen was considered a strategic priority for investment in public health and considered superior to early detection at the population level7,10.
On the other side, the early detection strategy seems to identify a greater number of melanomas at an early stage but also leads to the detection and treatment of a much larger number of benign lesions, resulting in higher costs and a slight negative impact on quality of life compared with the absence of intervention in some scenarios. Thus, the higher proportion of melanomas detected may not offset the risk of overdiagnosis and unnecessary treatments, economic burdens, and the slight negative impact on quality of life7.
Regarding protective clothing, Yusufov et al. states that it is one of the most validated methods of photoprotection and that, together with the use of sunscreen, it may be more effective in preventing and reducing sunburns than the use of sunscreen alone14.
Navarro-Bielsa et al. concluded that clothing was the least commonly used measure in their population (always or habitually, 22.8%). The melanoma group used clothing the least (13.7%) followed by the BCC group (22.2%), control group (26%), and SCC group (28.8%)15.
The importance of combining different forms of photoprotection is highlighted, and it seems that none of these strategies should be viewed in isolation, but rather as part of an integrated set of preventive measures16.
Several studies focus on the impact that educational and awareness interventions have on sun protection behaviors with the aim of reducing the risk of skin cancer or improving early detection. Many of these approaches make use of educational materials in print (such as leaflets) or digital (such as websites or short message service [SMS] messages), often including counseling – carried out by telephone, in person (by health professionals or genetic counselors), or integrated into structured programs.
Durand et al. suggest that ABi could be more effective in reducing sun exposure and improving sun protection, especially in groups with lower education levels and young adults. Emmons et al. also found a significant increase in the use of hats and sunscreen in the group that received biometric feedback, that is, the intervention group that viewed skin damage caused by exposure to UV radiation17.
On the other hand, other studies in the literature cited by Durand et al. show mixed results in the comparison between ABi and HBi: some report greater effect of ABi, others no difference, or even a greater effect of HBi. This underlines the need for further research on which approaches work best for different populations and behaviors11.
Byrne et al. highlights that, even in a group with high knowledge (medical students), positive attitudes toward tanning are associated with risk behaviors. High knowledge did not automatically translate into safe behaviors, and in fact, could be positively correlated with risk behaviors. This supports the idea that campaigns should focus more on changing attitudes and social norms (especially regarding tanning) rather than only on increasing knowledge17. Durand et al. incorporates the change in social norms regarding tanning into their ABi intervention, which may explain part of its effectiveness in reducing sun exposure. Aleo et al. also found low levels of knowledge in Italy, but behavioral outcomes were moderate/sufficient, suggesting that the knowledge–behavior relationship is complex and influenced by other factors such as attitudes and risk perception11.
Regarding tanning, Byrne et al. identified positive attitudes toward tanning as a key driver of risk behaviors. Durand et al. states that tourists seek the sun and are particularly sensitive to the positive image of tanning, suggesting why ABi may be effective by highlighting the negative image of photoaging. Therefore, the persistence of positive attitudes toward tanning, despite the known risks, is a challenge for melanoma prevention11,18.
THEORETICAL MODELS
Theoretical models have been used to underpin interventions promoting sun protection behaviors, namely the Transtheoretical Model (TTM), the Theory of Planned Behavior (TPB), and the Health Belief Model (HBM).
The TTM is a model of intentional behavior change, composed of five stages: precontemplation, contemplation, preparation, action, and maintenance.
Yusufov et al. found that individuals successful in maintaining behavior consistently use more processes of change, like increasing awareness and stimulus control than those who relapse or do not change14.
The TPB argues that behavior is determined by behavioral intention.
Durand et al. refers to the use of TPB; however, they do not provide detailed information about practical application in the study, which limits the assessment of its effectiveness11.
The HBM seeks to explain and predict health behaviors based on individual beliefs and perceptions about disease and the benefits of preventive action.
Variables such as age, gender, and previous experiences also influence these perceptions. Aleo et al. applied a questionnaire based on the HBM to assess perceived melanoma risk, concern, knowledge, and protective behaviors, with the data used for social marketing19.
The HBM emphasizes that factual knowledge alone is insufficient. Effective interventions must act on perceptions, motivate action, and provide realistic strategies for adopting healthy behaviors.
PRACTICAL IMPLICATIONS
Across studies, BC interventions seem to improve sun-protective behaviors, particularly sunscreen use and awareness of melanoma risk.
Educational and counseling interventions demonstrated variable effectiveness in translating knowledge into sustained behavior change. Several studies highlighted that increased knowledge alone does not necessarily reduce risky behaviors, especially in populations with persistent positive attitudes toward tanning.
Sun protection campaigns could therefore go beyond generic messages focused exclusively on oncological risks. The inclusion of arguments related to the aesthetic effects of sun exposure, such as photoaging, may also prove effective, especially among younger population groups who may value esthetics more or who have lower levels of education.
Future interventions can, therefore, focus on modifying positive attitudes toward tanning, as well as transforming the social norms that promote it.
The promotion of regular and daily use of sunscreen should also be a priority in public health strategies, as it is a cost-effective measure that contributes significantly to the reduction of melanoma incidence.
It is also important to recognize that patterns of sun exposure vary according to lifestyle and occupational context. Effective prevention campaigns should be tailored to specific populations, for example, taking into account that outdoor workers exhibit different risk behaviors than tourists engaging in more recreational outdoor activities.
Furthermore, it is necessary to support not only the initial adoption but also the maintenance of protective behaviors. The application of theoretical models can be useful in this context, highlighting the importance of processes of change which contribute to the sustained maintenance of preventive behaviors. Applying these models in practical interventions offers a more personalized and effective approach to behavior modification, especially if perceptions of risk, perceived barriers, and individual incentives for behavior change are taken into account20.
Raising population awareness requires an integrated effort and approach among different stakeholders. We must recognize that health professionals play a fundamental role in educating the population about the risks of sun exposure. It is equally important to ensure that future health professionals are properly prepared to inform and guide the population, ideally through strategies adapted to individual characteristics.
Overall, BC interventions show moderate-strength evidence for improving preventive behaviors, though long-term adherence and clinical outcomes remain insufficiently studied.
BC and technology, mobile applications, online interventions, and multimedia resources (T)
Regarding the use of technology in primary prevention, the most recurring themes include sending text messages to mobile phones (SMS), smartphone applications (apps), and web-based interventions and multimedia resources.
Text messages (SMS) appear to be a flexible way to support the promotion of sun protection behaviors. Studies address their use for sending reminders or educational messages related to sun protection or skin self-examination. They often include elements of personalization based on participant characteristics, such as gender, risk factors, and previous history of sunburns. Some studies also evaluate the use of interactive messages, requiring participant response or interaction with links to websites, and the effectiveness of different sending frequencies (daily, weekly, and monthly).
Horsham et al. suggest that text message interventions could lead to an increase in sun protection and a decrease in sunburns among young adults, with effects lasting up to 6 months after follow-up21.
On the other side, Youl et al. demonstrated that SMS intervention did not appear to have a significant effect on the proportion of participants reporting sunburns, although all groups reported decreasing rates.
Horsham et al. and Youl et al. found that the acceptability of these interventions is generally high, with most participants reading the messages sents; therefore, the role of text message interventions in melanoma prevention is promising21.
Horsham et al. also found a preference for interactive messages, which require a response from the recipient, and an ideal frequency of three messages per week. It would be interesting to understand whether offering the individual option to personalize reminders, frequency, or message reception time influences primary prevention behaviors, as well as whether messages with positive reinforcement responses, such as praise, requiring feedback, and responses from participants, could be truly more effective21.
Interestingly, it was observed that text messages may encourage conversations about sun protection among participants and their friends or family, involving a significant proportion of the sample21,22.
Regarding smartphone applications, they can include features such as notifications or reminders for skin self-monitoring and provide prevention and awareness information. For example, the SunSmart Global UV app provides sun protection alerts based on real-time and forecast UV levels, adapted to the user’s location.
Some studies have also focused on online interventions and multimedia resources (computer-based interactive programs) to provide information and promote behavioral changes. Manne et al. found that the online intervention “mySmartSkin” in melanoma survivors was associated with a beneficial impact on skin self-examination and sun protection behaviors, with some effect over time23.
Glazebrook et al. demonstrated that the interactive program “Skinsafe,” which uses images, animation, and sound to reinforce learning, reported positive changes in at least one photoprotective behavior, most frequently related to the use of protective clothing, although the average study quality was considerate moderate24.
Bowen et al., in 2017, found that the web intervention “Suntalk” for families of melanoma survivors favorably changed the frequency of communication about cancer risk among family members. It was also linked to increased levels of protection behaviors, although website usage frequency was not associated with outcomes14.
In addition, technology is being used in the development of new risk assessment tools that can be implemented in primary care settings, for example, through tablets in waiting rooms, to provide personalized prevention strategies. Teledermatology and UV sensors that can be used in clothing are other technologies with potential to improve melanoma prevention and early detection, although evidence on their effectiveness and implementation is still limited, according to Singh et al.20,25.
Technology-based approaches demonstrated high acceptability and modest short-term improvements in sun-protective behaviors. Evidence regarding SMS interventions was mixed: some studies reported reductions in sunburns and improved protection behaviors, while others showed no significant differences compared to controls.
Web-based and multimedia interventions appeared beneficial in specific populations, such as melanoma survivors and high-risk individuals, particularly for skin self-examination and communication about risk. However, engagement levels varied.
Overall, the evidence for technology-based interventions can be considered promising but heterogeneous, with outcomes largely dependent on user engagement and population characteristics. Equity and accessibility remain key limitations.
BC and the provision of genetic or personalized information on individual risk of developing melanoma (G)
The provision of genetic or personalized information on individual risk is also explored as a potential strategy to improve melanoma prevention.
This approach is essentially based on the analysis of common genetic variants, such as those in the MC1R gene, or on the use of polygenic risk scores based on multiple genes. The goal is to communicate risk individually to participants, often through educational materials and counseling. Ultimately, the use of this personalized information aims to promote more effective prevention and detection behaviors by increasing risk awareness.
Several studies seek to evaluate whether communicating personalized risk effectively leads to changes in sun protection and detection behaviors.
Lacson et al. demonstrated self reported improvements in specific prevention and detection behaviors, particularly among participants identified as having higher risk, including those with a family history of melanoma. Reported behaviors included increased use of sunscreen, increased frequency of professional skin examinations, increased frequency of skin self-examinations, and increased use of sunglasses and protective clothing26.
On the other hand, Lacson et al. report that the personalized intervention did not have a significant impact on reported preventive behaviors among participants at medium or low risk, suggesting that the information may be more relevant for high-risk individuals25.
Smit et al. and Lacson et al. demonstrated the feasibility and acceptability of the population in receiving personalized information on genomic melanoma risk. However, Hay et al. reported heterogeneous results regarding interest in and adherence to genetic testing based on demographic and socioeconomic factors, such as ethnicity and education level, indicating that non-Hispanic white and more educated populations could be more likely to show interest9,26,27.
Studies evaluating the communication of personalized or genetic melanoma risk show therefore mixed results. While high-risk individuals demonstrated some potential improvement in preventive and detection behaviors, medium and low risk groups showed little or no behavioral change.
Most studies state that personalized risk communication was feasible and did not increase anxiety or risk behaviors28. However, differential interest and uptake across socioeconomic and ethnic groups raise concerns about equitable implementation. Altogether, the evidence suggests selective effectiveness, which may indicate more benefit among high-risk populations, but limited impact at the population level.
CHEMOPROTECTIVE AGENTS (AQ)
Some studies also consider chemoprevention as a promising approach in melanoma prevention, which involves the use of drugs or natural agents with the aim of reducing the risk of developing the disease.
Pulumati et al. and Yan et al. investigated the chemopreventive potential of aspirin and other non-steroidal anti-inflammatory drugs in the context of cutaneous melanoma. The authors explored the possible biological mechanisms underlying the action of aspirin, namely the inhibition of the nuclear factor kappa B signaling pathway and cyclooxygenase (COX) enzymes, especially COX-2, whose expression has been associated with malignant cell progression29,30.
The studies highlight the need for more large-scale prospective studies with diverse populations and well-structured methodologies, which would allow clarification of this relationship and provide more robust clinical guidance.
On the other hand, Serini et al. highlight the potential of long-chain n-3 polyunsaturated fatty acids (LC n-3 PUFAs), consumed through the diet, in melanoma prevention. These fatty acids appear to exert some beneficial effects when used in combination with conventional therapies or as vehicles for drug delivery, being therefore more relevant for treatment or for enhancing existing therapeutic efficacy. Specifically in melanoma, LC n-3 PUFAs may inhibit tumor cell growth and induce apoptosis, mechanisms that may also be associated with the reduction of COX-2 expression5.
The hypothesis that LC n-3 PUFAs could act as chemopreventive agents for melanoma is based on results obtained in preclinical studies, as well as preliminary epidemiological observations. These data are complemented by the identification of multiple molecular mechanisms through which these compounds may exert a sustained protective effect against melanoma development. However, it is important to emphasize that the chemopreventive potential of LC n-3 PUFAs still requires validation through rigorously conducted human studies to confirm the benefits suggested by initial research.
Therefore, evidence supporting chemoprevention remains weak and inconclusive. While aspirin and LC n-3 polyunsaturated fatty acids have biologically plausible mechanisms and show promise in preclinical studies, human data are inconsistent and insufficient to support clinical recommendations. Current findings highlight the need for rigorously designed prospective studies before chemoprevention can be considered a viable preventive strategy.
Limitations and suggestions
Among the four categories, BC interventions currently have the strongest evidence base, particularly for promoting sunscreen use, whereas T and G interventions show context-dependent effectiveness and CQ strategies remain largely experimental. Across all categories, most outcomes rely on self-reported behaviors rather than long-term clinical endpoints, limiting conclusions regarding melanoma incidence and mortality reduction.
Future research should prioritize standardized outcome measures, and equitable intervention strategies that address social norms and behavioral maintenance rather than knowledge alone.
The use of standard erythemal doses measured by devices can assess sun exposure more accurately than self-reporting. Changing the data collection method from in-person interviews to online questionnaires may also potentially reduce social desirability bias.
It would also be interesting to study younger populations, who appear more prone to risk behaviors, and male populations, who are underrepresented in several studies. Additionally, populations with lower educational levels should be considered, along with how to personalize interventions for different educational levels.
In older populations, it would be valuable to conduct more studies on how to change behavioral habits in this age group, since providing personalized genetic information did not appear to be effective, nor did increasing general knowledge, according to Crowder et al.31.
Melanoma prevention requires a multifaceted approach; therefore, training general practitioners to identify higher-risk groups and provide more effective personalized interventions would be valuable. However, given that some of the main barriers to implementing primary prevention activities in primary healthcare include limited consultation time and competing demands on professionals, there is a need for future research on the feasibility and acceptability of integrating personalized, risk-based prevention strategies, and early skin cancer detection into primary care models.
Most studies have a follow-up period of up to 1 year, which may not be sufficient to assess the effectiveness and maintenance of sun protection behaviors. Studies with longer follow-up periods would therefore be important in the future to evaluate the efficacy of primary prevention strategies.
Conclusion
Melanoma prevention is a global public health priority due to its high incidence and mortality, particularly in populations with higher sun exposure. The literature addresses various primary prevention strategies, including behavioral counseling and health education, the use of technology, the provision of genetic information, and the exploration of chemoprotective agents. Interventions aimed at modifying risk behaviors, combined with awareness strategies and innovative technologies, can contribute significantly to reducing melanoma incidence, especially when tailored to the specific needs of population subgroups.
On one hand, behavioral counseling, education, and population awareness to adopt sun protection behaviors have been shown to be crucial components of prevention strategies. Regular use of sunscreen remains the most accessible and effective preventive measure for primary melanoma prevention, and studies indicate that it can significantly reduce melanoma incidence, representing a cost-effective public health strategy.
Additionally, education and awareness, whether through printed or digital educational campaigns, have an important impact on modifying behaviors. However, the effectiveness of these interventions may be limited by factors such as individual risk perception and cultural attitudes, such as the a esthetic value placed on tanning.
The use of theoretical models, such as the TTM and the HBM, in the design of behavioral change strategies has proven fundamental for understanding the psychological processes involved in adopting sun-protective behaviors.
Incorporating technology into melanoma prevention interventions has also proven to be a promising strategy, particularly among young populations with access to technology. Sending text messages (SMS) and developing mobile applications promote preventive behaviors, such as sunscreen use, skin self-examinations, and adoption of real-time photoprotection practices tailored to user characteristics and environmental conditions.
Multimedia resources, such as interactive online websites, have also demonstrated utility in promoting health literacy and improving adherence to protective behaviors, such as performing skin self-exams. Through visual and interactive elements, these tools contribute to better understanding and retention of information by the population.
Subsequently, the provision of personalized information about genetic risk for melanoma is an emerging area of research with great potential to improve prevention. However, the effectiveness of this approach appears limited in individuals with medium or low risk, and adherence may be influenced by demographic and socioeconomic factors. The provision of genetic information should be carried out cautiously to avoid low-risk individuals becoming complacent about preventive measures.
Finally, chemoprevention, especially the use of chemoprotective agents such as aspirin, has been explored in some studies, although the results remain inconclusive and do not allow for clear practical recommendations.
It is also important to emphasize that successful implementation of melanoma prevention strategies requires an integrated approach. Therefore, collaboration between healthcare professionals, researchers, and public health officials is essential in developing targeted campaigns and interventions tailored to the specific characteristics of each population group.
Reducing melanoma incidence requires collective responsibility and continuous, multifaceted effort. Future studies should focus on larger participant numbers and longer follow-up periods to determine the best and most effective strategies for behavioral change that are demonstrably long-lasting and sustained, ultimately reflecting a real decrease in melanoma incidence.
Funding
None.
Conflicts of interest
None.
Ethical considerations
Protection of human subjects and animals. The authors declare that no experiments on humans or animals were performed for this research.
Confidentiality, informed consent, and ethical approval. This study does not involve personal patient data, medical records, or biological samples, and does not require ethical approval. SAGER guidelines do not apply.
Declaration on the use of artificial intelligence (AI). The authors declare that no generative artificial intelligence was used in the writing or creation of the content of this manuscript.
Supplementary data
Supplementary data are available at DOI: 10.24875/PJDV.25000077. These data are provided by the corresponding author and published online for the benefit of the reader. The contents of supplementary data are the sole responsibility of the authors.
