Introduction
Chronic urticaria is a distressing condition commonly encountered by dermatologists globally, characterized by recurrent transient itchy wheals and/or angioedema lasting for more than 6 weeks. It can be further categorized into spontaneous or inducible.
The prevalence of chronic spontaneous urticaria (CSU) is estimated to be around 0.5-1% of the general population.1 CSU typically peaks around the fourth decade of life and is more common in females than in males.
CSU occurs due to the interplay of various causative factors that act synergistically or sequentially, either by independent or interlinked mechanisms. This results in mast cell activation and release of preformed vasoactive mediators and newly synthesized pro-inflammatory molecules.2
Even though the pathomechanism of CSU is multifarious, autoimmunity plays a significant role, further justified by the association of CSU with other auto-immune conditions such as auto-immune thyroid disease,3 vitiligo, pernicious anemia, and rheumatoid arthritis.4 The most accepted pathogenic mechanism of CSU is the presence of autoantibodies on a background of chronic inflammation. Immunoglobulin E (IgE) antibodies against auto-antigens, namely interleukin (IL)-24 or thyroperoxidase (type 1 autoallergic CSU), are detected in several patients, and immunoglobulin G autoantibodies against IgE and FcꜪRI (type 2 auto-immune CSU) are detected in about 30-50% of the patients.5 The binding of autoantibodies to mast cells results in complement activation, and the generation of C5a anaphylatoxin facilitates or augments mast cell degranulation.6 This leads to the release of histamine, proteases, cytokines, and other metabolites of arachidonic acid, thus leading to chronic inflammation.
Moreover, abnormal innate immunity, dysregulated intracellular signaling pathways in basophils and mast cells, and concurrent activation of the inflammatory response and coagulation system also contribute to the development of CSU.2,7,8
CSU is known to be associated with low-grade chronic inflammation, as depicted by mast cell degranulation in the skin, infiltration of T cells, eosinophils, and neutrophils, as well as elevated levels of pro-inflammatory cytokines in circulation.9 Inflammation plays a crucial role in connecting the immune system with hypercholesterolemia, which is a contributing factor to the elevated risk of cardiovascular disease.10 The levels of pro-inflammatory cytokines reflect the severity of lipid abnormalities.8 Symptoms of auto-immune diseases were found to be improved by cholesterol-lowering treatments such as a low-fat diet or statins.11
Moreover, increased body mass index (BMI), or obesity, frequently found in CSU patients, can further lead to changes in lipid metabolism. Adipose tissue acts as an active endocrine organ, releasing pro-inflammatory cytokines that may exacerbate the skin condition and alter the lipid profile. Mast cells have been found to cause endothelial inflammation and alter the lipid profile, thereby promoting the development of atherosclerosis.12–15
As chronic inflammatory skin diseases are recognized as risk factors for dysmetabolic syndrome, it is plausible that CSU also plays a role in the development of dyslipidemia.16,17 Elevated levels of pro-inflammatory cytokines such as tumor necrosis factor-α and IL-618 can cause dyslipidemia by reducing the breakdown and removal of cholesterol19 and by inhibiting the activity of adipocyte lipoprotein lipase,20 respectively.
Cytokines play a role in elevating fatty acid synthesis and reducing their oxidation within the liver. They also stimulate the breakdown of fats in adipose tissue, leading to increased triglyceride (TG) synthesis in the liver. Greater TG availability results in heightened production and release of very low-density lipoprotein (VLDL).21
Henceforth, CSU and dyslipidemia might be connected through an underlying inflammatory process or immune system dysregulation. A recent study conducted in Germany by Weller et al. revealed that metabolic disorders impacting lipoproteins were often cited as comorbidities in individuals with chronic urticaria,22 and a study by Viswanath et al. showed TG to be significantly elevated in patients with CSU.23 Furthermore, the composition and distribution of high-density lipoprotein (HDL) particles are reported to be significantly altered in CSU, affecting their ability to modulate immune cell responses.24 Low-density lipoprotein (LDL) is more readily absorbed by smooth muscle cells and macrophages when it binds to the leftover granules of mast cells.14
However, fewer studies have evaluated the exact potential link between CSU and dyslipidemia. Hence, after thoroughly going through the conflicting literature on dyslipidemia and CSU, we devised a plan to assess serum lipid levels in CSU patients and determine whether the association exists in our demographics.
The objectives of this study are to compare the lipid profiles of patients with CSU and healthy controls, to identify which lipid parameter is most altered in CSU, and to determine the age and sex group among CSU patients most commonly affected by dyslipidemia.
Methods
This cross-sectional study included 30 cases of CSU and 30 age- and sex-matched healthy controls seen at the dermatology outpatient department of a tertiary care hospital.
Individuals aged 15-45 years who provided informed consent were included, with cases comprising those with a clinical diagnosis of CSU and controls free of skin or systemic diseases. Exclusion criteria included patients with dyslipidemia, conditions predisposing to dyslipidemia (such as diabetes, hypothyroidism, chronic kidney or liver disease, and other endocrine disorders), those on lipid-lowering medications (such as statins or fibrates), and individuals taking drugs that could alter serum lipid levels (such as diuretics, retinoids, anabolic steroids, glucocorticoids, estrogens, cyclosporine, β-blockers, and antipsychotics). In addition, patients with chronic skin or rheumatological diseases, a family history of dyslipidemia or myocardial infarction, and pregnant or breastfeeding women were excluded.
Consent was obtained from the subjects after explaining the purpose of the research. Under sterile conditions, blood samples were collected in a tube without an anticoagulant after 10 h of fasting and then sent for analysis.
Serum lipid profile was conducted by an autoanalyzer and included total cholesterol (TC), TG, HDL-C, LDL-C, VLDL, and cholesterol/HDL ratio (TC/HDL). Normal reference values are as follows: < 200 mg/dL for TC, < 150 mg/dL for TG, > 40 mg/dL for HDL, < 130 mg/dL for LDL, < 30 mg/dL for VLDL, and < 3.5 for the TC/HDL ratio.
Data obtained were tabulated and assessed by IBM Statistical Package for Social Sciences V20 software. Continuous variables were outlined using frequency, mean, and standard deviation. Means among groups were compared using an independent t-test, and proportions were compared using the X2 test. A p < 0.05 was considered statistically significant.
This study was reviewed and approved by the institutional ethics committee of the tertiary care hospital where the research was conducted (IEC No: IEC/KMCH/2023/71).
Results
Our study included 30 CSU cases (12 males and 18 females) and 30 age- and sex-matched controls (15 males and 15 females) between 15 and 45 years of age. The overall mean age of cases was 29.4 ± 8.1 years, whereas that of controls was 30.3 ± 8.6 years.
Dyslipidemia was detected in 53.3% of CSU cases and 36.6% of controls (p = 0.299), with CSU cases having the highest number of individuals with alterations and higher mean values within the TG and VLDL.
We observed elevated TG in 50% (15 patients) of CSU cases compared to 26.6% (8 patients) of controls in our study (Table 1). Mean levels of TG were remarkably higher in CSU cases (161.1 ± 74.3) than in controls (128.9 ± 34.3), with p = 0.036 (Table 2). VLDL was elevated in 12 patients (40%) with CSU, compared to 7 (23.3%) in controls. Statistically significantly higher values of VLDL were noted in CSU cases (33.7 ± 20.6) compared to controls (21.5 ± 8.93), with p = 0.004 (Table 2). A high cholesterol/HDL ratio was observed in 16 CSU patients (53.3%) and in 11 controls (36.6%), but the mean value of this ratio was not significantly different (3.83 ± 0.803 vs. 3.75 ± 0.82). No significant differences were observed in the number of patients with changes in TC, LDL, or HDL between patients and controls. Furthermore, the mean levels of TC, HDL, LDL, and TC/HDL between patients and controls did not differ statistically significantly in our investigation (Tables 1 and 2).
Table 1. Number of cases and controls with altered serum lipids and lipoproteins
| Lipid parameter | CSU (%) | Controls (%) | p |
|---|---|---|---|
| Cholesterol | 6 (20) | 5 (16.6) | 1.000 |
| LDL | 4 (13.3) | 3 (10) | 1.000 |
| HDL | 5 (16.6) | 7 (23.3) | 0.748 |
| TC/HDL | 16 (53.3) | 11 (36.6) | 0.299 |
| Triglycerides | 15 (50) | 8 (26.6) | 0.110 |
| VLDL | 12 (40) | 7 (23.3) | 0.267 |
|
TC: total cholesterol; LDL: low density lipoprotein; HDL: high density lipoprotein; TG: triglycerides; TC/HDL: total cholesterol/high density lipoprotein; VLDL: very low density lipoprotein; CSU: chronic spontaneous urticaria. |
|||
Table 2. Mean values of lipid profile among cases and controls
| Lipid profile | CSU cases (mean ± SD) | Controls (mean ± SD) | p |
|---|---|---|---|
| Cholesterol | 177.4 ± 31.4 | 170.2 ± 31.4 | 0.379 |
| LDL | 97.9 ± 24.5 | 99.3 ± 23.9 | 0.824 |
| HDL | 47.33 ± 8.84 | 46.10 ± 7.60 | 0.569 |
| TC/HDL | 3.83 ± 0.80 | 3.75 ± 0.82 | 0.702 |
| Triglycerides | 161.1 ± 74.3 | 128.9 ± 34.3 | 0.036 |
| VLDL | 33.7 ± 20.6 | 21.5 ± 8.93 | 0.004 |
|
TC: total cholesterol; LDL: low density lipoprotein; HDL: high density lipoprotein; TG: triglycerides; TC/HDL: total cholesterol/high density lipoprotein; VLDL: very low density lipoprotein; SD: standard deviation; CSU: chronic spontaneous urticaria. |
|||
In the CSU group, dyslipidemia affected 9 males (30%) and 7 females (23.3%), whereas in the control group, it affected 6 males (20%) and 5 females (16.7%) (Table 3).
Table 3. Sociodemographic profile among CSU cases and controls with dyslipidemia
| Sociodemographic profile | CSU cases with dyslipidemia (%) | Controls with dyslipidemia (%) | p |
|---|---|---|---|
| Male | 9 (30) | 6 (20) | 0.552 |
| Female | 7 (23.3) | 5 (16.7) | 0.748 |
| Total | 16 (53.3) | 11 (36.7) | 0.299 |
| Age groups 15-25 years 26-35 years 36-45 years Age (mean ± S.D) | 3 (10)8 (26.6)5 (16.7)31.56 ± 7.57 | 2 (6.7)4 (13.3)5 (16.7)32.36 ± 8.41 | 1.0000.3331.0000.700 |
|
SD: standard deviation; CSU: chronic spontaneous urticaria. |
|||
The mean age of CSU cases with dyslipidemia was 31.56 ± 7.57 years compared with 32.36 ± 8.41 in controls. Most cases of dyslipidemia in the CSU group with elevated TG and VLDL occurred in the 26-35 year age group (26.6%), followed by 36-45 (16.7%) and 15-25 years (10%), whereas the 36-45 year age group (16.7%) was the most affected in controls (Table 3 and Fig. 1).
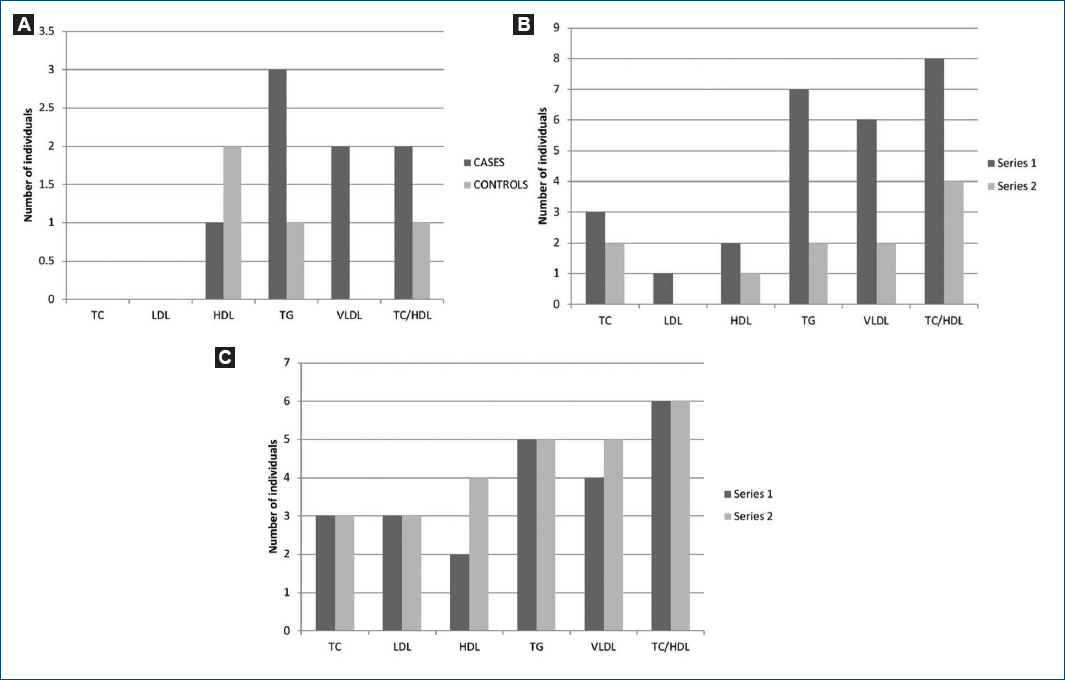
Figure 1. Altered lipid profile in different age groups. A: 15-25 year age group. B: 26-35 year age group. C: 36-45 year age group.
Discussion
Our sample of CSU, with the age of disease distribution between 15 and 45 years, a mean age of around 30, and a significant female predominance (18 patients), is in accordance with the previous studies on the demographics of CSU.25,26
Similar to the observations of Ye et al.,27 our study found a slight predominance of dyslipidemia in males compared to females among cases. The mean age of distribution among cases with dyslipidemia was 31.56 ± 7.57 years. Dyslipidemia showed the highest incidence in the 26-35 year age group, with the 36-45 and 15-25 year age groups following suit.
Dyslipidemia was present in 53.3% of cases, and the elevation in the mean serum TG was found to be statistically significant in cases (p = 0.036) when compared to controls. This observation is consistent with the study conducted by Vishwanath et al.23
There is a statistically significant elevation in the mean serum VLDL levels in cases compared to controls. However, the changes in TC, HDL, LDL, and TC/HDL were not statistically significant in cases compared to controls. These findings were in accordance with the observations of Vishwanath et al.,23 but are discordant with the results of studies done by Amin et al.,28 and Ayub et al.,29 who noted a significant difference in the mean levels of serum TC, LDL-C, and HDL-C in CSU patients compared to controls.
On the contrary, our results regarding the statistically significant elevation of mean TG and insignificant elevation of HDL also stand in discordance with a study by Yaldiz and Asil et al.30
Statistically significantly elevated levels of mean serum TG and VLDL were noted among cases compared to controls in our study, enforcing the role of CSU in the development of dyslipidemia. Hence, it is better to evaluate patients with CSU for dyslipidemia, thereby preventing its dreadful complications and ultimately improving life expectancy.
Limitations
The study is limited by its small sample size and the omission of BMI as a covariate.
Conclusion
Dyslipidemia, involving particularly TG and VLDL, is more frequent in CSU patients and at a slightly younger age, and is often underreported because it is clinically asymptomatic, which can result in inadequate management and an elevated risk of atherosclerosis, cardiac, and cerebrovascular complications. Therefore, early detection and proper management can decrease the likelihood of subsequent complications and enhance the patient’s quality of life.
Funding
None.
Conflicts of interest
None.
Ethical considerations
Protection of human subjects and animals. The authors declare that no experiments on humans or animals were performed for this research.
Confidentiality, informed consent, and ethical approval. The authors have followed their institution’s confidentiality protocols, obtained informed consent from all patients, and secured approval from the ethics committee. SAGER guidelines have been followed as applicable to the nature of the study.
Declaration on the use of artificial intelligence. The authors declare that no generative artificial intelligence was used in the writing or creation of the content of this manuscript.
