A 41-year-old male presented with an asymptomatic lesion on his groin that had been gradually enlarging over 5 years. On physical examination, a 12 × 7 cm slightly indurated, flesh-colored plaque with pedunculated nodules was observed in the left inguinal region (Fig. 1). Histopathological examination of a biopsy showed a tumor with diffuse infiltration of the skin and subcutaneous tissue composed of uniform and medium-sized spindle cells with a storiform or cartwheel pattern of growth (Fig. 2), consistent with dermatofibrosarcoma protuberans (DFSP). Staging showed no evidence of secondary lesions. Given the tumor’s size and risk of functional impairment, the patient was started on therapy with imatinib. At the 6-week follow-up, the lesion remained stable.
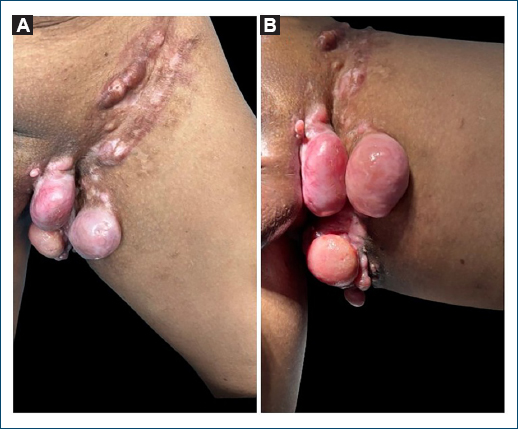
Figure 1. Clinical images with an indurated, flesh-colored plaque with several pedunculated nodules in the left inguinal region (A: frontal and B: medial views).
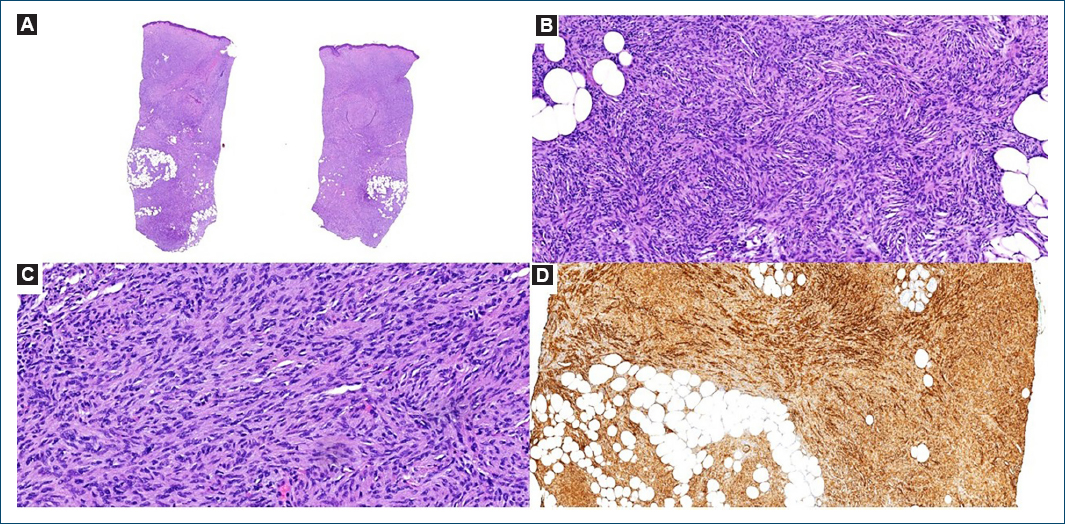
Figure 2. Dermatofibrosarcoma protuberans – low-power magnification with diffuse infiltration of the skin and subcutaneous tissue (A: H&E); uniform and medium-sized spindle cells with a storiform or cartwheel pattern of growth (B: H&E 100×); minimal atypia and no mitotic figures or necrosis (C: H&E 400×); the cells have diffused strong staining for CD34 (D: immunohistochemistry 100×).
DFSP is a rare, slow-growing, and locally aggressive soft-tissue tumor1. DFSP primarily affects adults, with a peak incidence between 30 and 50 years, and shows a slight male predominance1,2. The tumor most commonly occurs on the trunk, followed by proximal extremities and, less frequently, the head and neck1. Clinically, it presents as a firm, indurated, nodular, and flesh-colored or violaceous plaque that may initially resemble benign skin lesions, leading to delayed diagnosis3. Despite its indolent behavior, DFSP has a high propensity for local recurrence if not completely excised1,3. Wide local excision with histologically clear margins remains the treatment of choice4. Imatinib is an option for patients with unresectable, recurrent, and/or metastatic disease, as well as an alternative to radical surgery in select cases5. While metastasis is rare, recurrence poses significant challenges, requiring long-term follow-up1.
Funding
None.
Conflicts of interest
None.
Ethical considerations
Protection of humans and animals. The authors declare that no experiments involving humans or animals were conducted for this research.
Confidentiality, informed consent, and ethical approval. The authors have followed their institution’s confidentiality protocols, obtained informed consent from patients, and received approval from the Ethics Committee. The SAGER guidelines were followed according to the nature of the study.
Declaration on the use of artificial intelligence (AI). The authors declare that no generative artificial intelligence was used in the writing of this manuscript.
