Hand-foot-mouth disease (HFMD) is an acute infectious disease caused by enteroviruses, characterized by enanthem and maculopapular and/or vesicular cutaneous rash affecting the hands, feet, and perioral and perineal regions.1 Less commonly, atypical HFMD can occur with an exuberant widespread rash, increasingly associated with coxsackievirus A6.2–4
A healthy 11-month-old boy, with an epidemiological context of conjunctivitis at kindergarten, presented to the pediatric emergency department with a 3-day history of fever and 1-week history of enanthem and pruritic papulovesicular rash in perioral region, scalp, limbs, hands, and feet, with plaques and tense bullae on the thighs, extensor surfaces, and hands and feet, involving fingers (Figs. 1 A–C). Nasopharyngeal swab was positive for enterovirus/rhinovirus. Impetiginized viral rash and eczema herpeticum were considered and the patient started on antibiotic and antiviral medication.
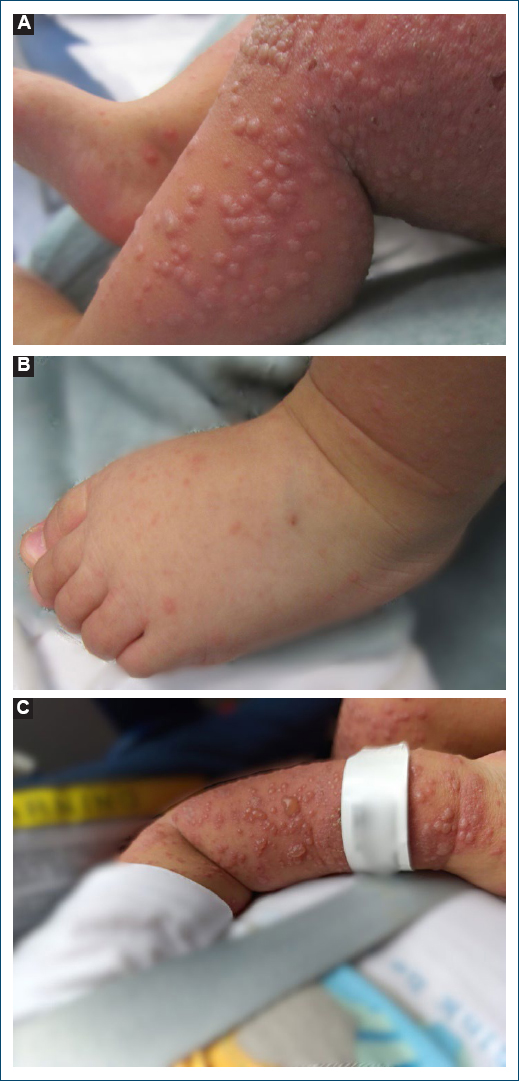
Figure 1. Clinical images. A: papulovesicular rash. B: hands and feet rash, involving the dorsum of feet and fingers. C: tense bubble in the extensor surface of the left arm.
The exuberance of the rash prompted a dermatology consultation. Considering the clinical presentation and laboratory findings, and after a typical skin biopsy (Fig. 2), the diagnosis of HFMD was made. The antibiotic and antiviral medication was discontinued, and the infant was discharged after 4 days. 2 weeks later, the skin lesions had resolved, but the child developed onychomadesis.
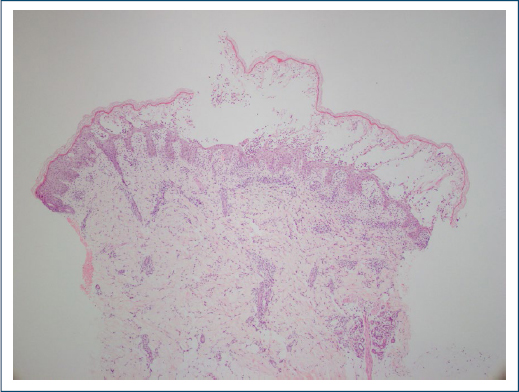
Figure 2. Skin biopsy, stained with hematoxylin-eosin, showed an intraepidermal vesicle with marked intracellular edema, focal superficial epidermal necrosis, with a mostly neutrophilic infiltrate, and a perivascular and interstitial mixed inflammatory infiltrate in the superficial dermis
While enterovirus infections in infants can vary in severity, coksackie A6 is often linked to characteristic lesions, including those on the hand and feet and onychomadesis,5 suggesting this patient may have been infected by this serotype, although it was not possible to confirm it.
This atypical presentation that delayed diagnosis, highlighting the need for clinicians to be aware of exuberant unusual clinical presentations and potential serious complications of HFMD, even in pediatric patients.4
Funding
None.
Conflicts of interest
None.
Ethical considerations
Protection of human subjects and animals. The authors declare that no experiments on humans or animals were performed for this research.
Confidentiality, informed consent, and ethical approval. The authors have followed their institution’s confidentiality protocols, obtained informed consent from all patients, and secured approval from the Ethics Committee. SAGER guidelines have been followed as applicable to the nature of the study.
Declaration on the use of artificial intelligence. The authors declare that no generative artificial intelligence was used in the writing or creation of the content of this manuscript.
