Introduction
Despite their rarity, angiosarcomas are among the more common forms of cutaneous sarcomas, ranking fourth after Kaposi’s sarcoma, dermatofibrosarcoma protuberans, and pleomorphic dermal sarcoma1,2. These tumors are highly aggressive and present significant diagnostic and therapeutic challenges due to their variable clinical presentations.
Three types of angiosarcoma have been identified: primary, associated with chronic lymphedema, and post-radiation1–3. The most common type is primary angiosarcoma (idiopathic or Wilson-Jones), which mainly affects Caucasian men over 70 years old. It usually presents on the head and neck regions as a single lesion resembling an innocent hematoma1,2. Angiosarcoma associated with chronic lymphedema presents as firm violaceous nodules or hardened plaques on a background of non-pitting edema; more than 90% of these cases are associated with mastectomy and lymph node dissection in women with breast cancer (Stewart-Treves syndrome)1,2. Lymphedema precedes the appearance of angiosarcoma in 4-27 years1–3. Post-radiation angiosarcomas manifest as infiltrating plaques or nodules in or near the irradiated area, approximately 6 years after treatment1–3.
Awareness among dermatologists is crucial for early diagnosis, as long-term survival largely depends on prompt radical surgery and adjuvant radiotherapy. This series describes the clinical and histopathological characteristics of the five cases of cutaneous angiosarcomas diagnosed over a period of 9 years in a dermatology department at a tertiary hospital in Lisbon, Portugal.
Case reports
Case 1
A 92-year-old Caucasian man presented with multiple violaceous patches, plaques, and nodules on the scalp (Fig. 1). Histopathologic examination from an incisional skin biopsy revealed an endothelial infiltrative tumor (Fig. 2). Immunohistochemistry was positive for CD31 and electroretinography (ERG). According to the 8th edition of the American Joint Committee on Cancer (AJCC) tumor, node, metastasis (TNM) staging system, the tumor was classified as stage I (T3N0M0). The patient underwent surgical excision but died 3 months later due to an unrelated infectious complication, before starting the proposed adjuvant radiotherapy.
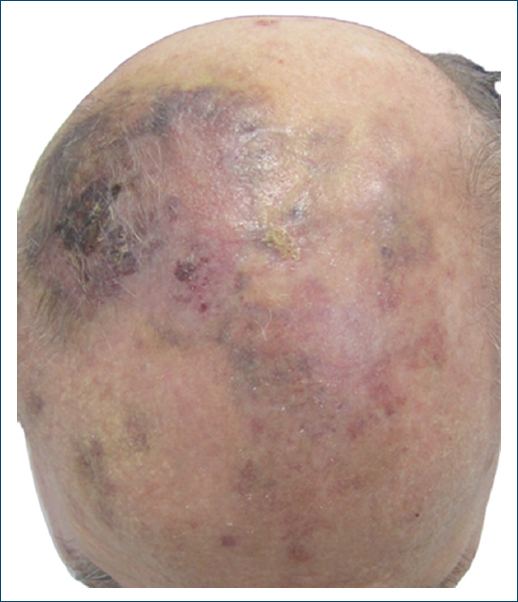
Figure 1. Physical examination showed multiple violaceous patches, plaques, and nodules on the scalp.
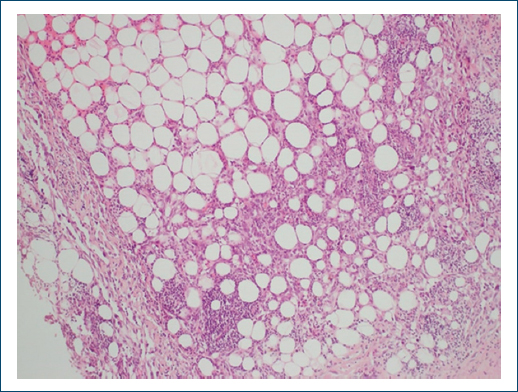
Figure 2. Histopathologic examination from an incisional skin biopsy reveals an endothelial tumor infiltrating the collagen bundles and adipose tissue (H&E, ×100).
Case 2
An 87-year-old woman with a history of breast cancer 17 years earlier, treated with conservative mastectomy and radiotherapy, presented with a violaceous nodule in the previously irradiated area (Fig. 3). Histopathologic examination of the surgical specimen revealed a tumor with diffuse proliferation in the dermis and subcutaneous tissue, irregular vascular clefts with fusiform endothelial cells, and cellular pleomorphism with round, epithelioid cells (Fig. 4). Immunohistochemistry was positive for CD31, podoplanin, ERG, and c-MYC. According to the AJCC (8th ed) TNM system, the tumor was staged as stage IA (T1aN0M0). Wide local excision was performed, and the patient remains alive and free of recurrence after 7 months of follow-up.

Figure 3. Physical examination showed a violaceous nodule in the left breast.
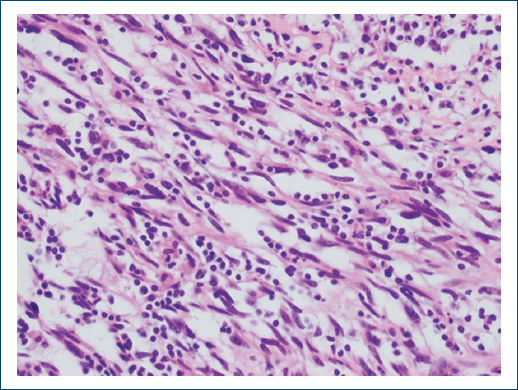
Figure 4. Histopathologic examination of the surgical specimen reveals a tumor with diffuse proliferation in the dermis and subcutaneous tissue and irregular vascular clefts (H&E, ×100).
Case 3
A 57-year-old female with chronic lymphedema of the right upper limb following mastectomy and lymphadenectomy for breast cancer 18 years earlier presented with multiple coalescent bleeding violaceous plaques and nodules on the inner aspect of the right arm (Fig. 5). Histopathologic examination from an incisional skin biopsy revealed a dense infiltrative tumor with epithelioid cells, the classic “fish in the creek” pattern, and pleomorphic, undifferentiated cells (Fig. 6). Immunohistochemistry was positive for CD31 and podoplanin. According to the AJCC (8th ed) TNM system, the tumor was staged as stage IV (T4N1M0). The patient also had a concurrent stage IIIA lung carcinoma. Given her poor performance status and the extent of cutaneous disease, she received best supportive care and died within 1 month due to sepsis.

Figure 5. Physical examination showed multiple coalescent bleeding violaceous plaques and nodules in the inner aspect of the right arm.
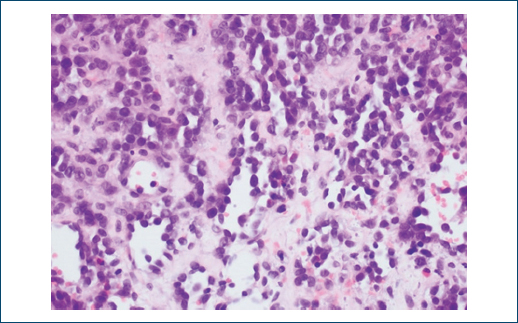
Figure 6. Histopathologic examination from an incisional skin biopsy revealed the classic “fish in the creek” sign and pleomorphic, undifferentiated cells with numerous mitoses (H&E, ×400).
Case 4
An 81-year-old female with chronic idiopathic lymphedema of the lower limbs presented with multiple friable coalescent bleeding nodules on the anterior aspect of the right leg (Fig. 7). Histopathologic examination from an incisional skin biopsy revealed an endothelial tumor with irregular vascular clefts and multilayering (Fig. 8). Immunohistochemistry was positive for CD31 and podoplanin. According to the AJCC (8th ed) TNM system, the tumor was staged as stage IB (T4 [multicentric] N0M0), compatible with localized inoperable disease. The patient was treated with radiotherapy and paclitaxel and survived for 13 months after diagnosis. The cause of death was unknown because of loss to follow-up.

Figure 7. Physical examination showed bleeding nodules on the anterior aspect of the right leg.
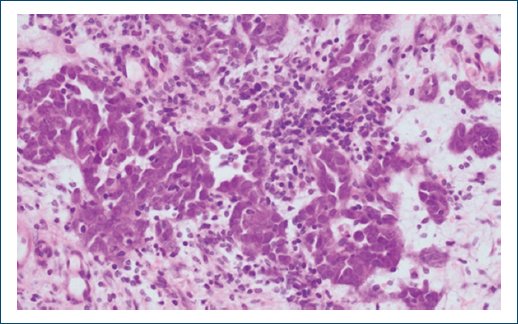
Figure 8. Histopathologic examination from an incisional skin biopsy revealed an endothelial tumor with irregular vascular clefts and multilayering (H&E, ×100).
Case 5
A 62-year-old male with a history of desmoplastic melanoma 12 years earlier and three local recurrences presented with a pink nodule in the previous surgical scar. Histopathologic examination of the surgical specimen revealed irregular vascular clefts dissecting between collagen bundles (Fig. 9). Immunohistochemistry was positive for CD31. According to the AJCC (8th ed) TNM system, the tumor was staged as stage IA (T1aN0M0). The patient underwent surgery, radiotherapy, and paclitaxel treatment. Despite these interventions, surgical margins remained positive, with local recurrences and locoregional lymph node involvement over time. He subsequently received systemic therapy with gemcitabine, doxorubicin, and pazopanib, but was later lost to follow-up and died 6 years and 5 months after diagnosis, with an unknown cause of death.
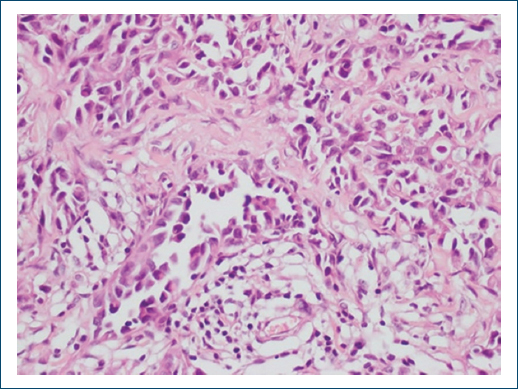
Figure 9. Histopathologic examination of the surgical specimen revealed irregular vascular clefts dissecting between the collagen bundles (H&E, ×100).
Results
We identified five cases of cutaneous angiosarcomas: two idiopathic (40%), two associated with chronic lymphedema (40%), and one post-radiation (20%). There were three female (60%) and two male (40%) patients. The mean age of our patients was 75.8 (standard deviation [SD] 13.8; range 57-92) years. The tumors were found in various locations, including the breast, trunk, limbs, and scalp, presenting as erythematous and violaceous patches, plaques, and nodules. Our analysis revealed a mean follow-up of 20 months and a mean overall survival of 23.5 months. Four out of the five patients (80%) died during the follow-up period.
Discussion
In our sample, the two most common types of cutaneous angiosarcoma were primary angiosarcoma and angiosarcoma associated with chronic lymphedema, followed by post-radiation angiosarcoma. These results differ from the literature, which most frequently reports primary angiosarcoma, followed by post-radiation angiosarcoma, and angiosarcoma associated with chronic lymphedema. The average age of our patients was consistent with data from the literature, indicating that most cases occur in elderly patients. Angiosarcomas are more common in males, but in our study 60% of the patients were female. The locations described in our analysis are consistent with those reported in the literature, although the most common location is the head and neck region, where we found only one tumor. Our study showed a mean overall survival of 23.5 months, corresponding to a 9-year survival rate of 20%, which is higher than the 5-year survival rate of 12-34% reported in the literature. These discrepancies are probably related to the small size of our sample.
The first case corresponds to the classic presentation of primary angiosarcoma, highlighting the importance of maintaining a high level of suspicion for persistent erythematous and violaceous lesions in the head and neck region in elderly patients. These lesions can initially be presumed to be benign or traumatic, especially in an elderly population commonly taking antiplatelet or anticoagulant drugs.
The second case is also a typical presentation to keep in mind, emphasizing the importance of suspecting cutaneous neoplasms in patients who have undergone radiotherapy for breast cancer. The main differential diagnoses to consider in this setting are basal cell carcinoma (the most common tumor), angiosarcoma, and atypical vascular lesions of the breast4. Differentiating between the latter two is challenging, with the presence of positive c-MYC favoring the diagnosis of angiosarcoma, stressing the importance of immunohistochemistry. Notably, the incidence of post-radiation angiosarcomas is increasing, while the incidence of angiosarcoma associated with chronic lymphedema, mainly seen following lymphadenectomy for breast cancer (Stewart-Treves syndrome), is decreasing. This reduction is attributed to the adoption of more conservative surgical techniques, combined with radiotherapy, for breast cancer.
The third and fourth cases are classic, from both a clinical and histopathological perspective. Clinically, the appearance of erythematous and violaceous skin lesions on a background of chronic lymphedema should always raise suspicion for angiosarcoma and prompt a biopsy. Histopathologically, the “fish in the creek” sign (free-floating endothelial cells within the vascular lumen) in the third case is considered a unique histologic pattern of cutaneous angiosarcoma5, and the multilayering in the fourth case is also typical.
The fifth case is the one showing the least common characteristics, considering the young age at presentation, the location on the back, and the history of recurrent desmoplastic melanoma in the affected site. In fact, a revision of the initial surgical specimens concluded that the lesions previously interpreted as melanoma were probably poorly differentiated angiosarcomas, misdiagnosed in an era when immunohistochemistry was not widely available. This case illustrates the clinical and histopathological diagnostic challenges of angiosarcomas.
Angiosarcomas pose two major challenges: clinical and histopathological diagnosis. Clinically, they can present as deceptively benign-appearing lesions, often in non-specific locations. Histopathologically, despite typical features, not all specimens reveal these changes6. The use of vascular markers in immunohistochemistry, including CD31, ERG, CD34, and Fli-1, is crucial for diagnosis6. ERG is currently considered the most sensitive and specific marker for angiosarcoma7.
Despite aggressive multimodal therapy, angiosarcomas have a poor prognosis, with a 5-year survival rate of 12-34%1,8. Early radical surgery followed by adjuvant radiotherapy appears crucial for improving outcomes. However, the high recurrence rate highlights the need for vigilant follow-up and possibly novel therapeutic approaches, including experimental therapy with propranolol, pembrolizumab, and the triple combination of pioglitazone with rofecoxib and trofosfamide9–11.
Our results illustrate the wide range of clinical presentations of cutaneous angiosarcomas and their diagnostic challenges. Furthermore, they corroborate literature data, indicating that these tumors have a very poor prognosis. However, this is a study with a small number of patients and potential selection biases, so results should be interpreted cautiously. Further research with larger, more diverse cohorts is needed to validate these observations.
Conclusion
Cutaneous angiosarcomas are aggressive endothelial tumors with significant clinical and histopathological variability. This case series emphasizes the need for heightened awareness among dermatologists and oncologists regarding the diverse presentations of angiosarcomas. Early diagnosis and aggressive treatment are pivotal in managing these tumors, although the prognosis remains poor. Further research into novel therapeutic strategies and better diagnostic markers is essential to improve outcomes.
Funding
None.
Conflicts of interest
None.
Ethical considerations
Protection of human subjects and animals. The authors declare that no experiments on humans or animals were performed for this research.
Confidentiality, informed consent, and ethical approval. The authors have followed their institution’s confidentiality protocols, obtained informed consent from all patients, and secured approval from the Ethics Committee. SAGER guidelines have been followed as applicable to the nature of the study.
Declaration on the use of artificial intelligence (AI). The authors declare that no generative artificial intelligence was used in the writing or creation of the content of this manuscript.
