Introduction
Onychomycosis, a chronic fungal infection affecting finger and/or toenails, constitutes 18.40% of onychopathies and about 30% of mycotic cutaneous infections. It can be dermatophytic or non-dermatophytic in origin. Although not life-threatening, onychomycosis constitutes an important public health problem because of its high prevalence and associated negative consequences for patients, such as pain, and can potentially undermine work and social lives.
The five clinical types reported are distal lateral subungual onychomycosis (DLSO), superficial white onychomycosis, proximal subungual onychomycosis (PSO), endonyx onychomycosis (EO), and total dystrophic onychomycosis (TDO)3. The onychoscopic signs usually observed in onychomycosis are a jagged proximal edge with spikes, longitudinal striae, a ruined appearance, and longitudinal ridges along the nail bed. However, these findings are limited to DLSO and TDO4. Hoffman and Driver emphasized the need for a correct identification of the causative organism apart from diagnosing the clinical type of onychomycosis5. However, the relationship between onychoscopic and clinical features and the causative organism is unknown. Hence, the primary objective of the study was to describe onychoscopic findings in patients with clinically suspected onychomycosis. Secondary objectives were (A) to determine the association between specific onychoscopic features and the clinical types of onychomycosis; and (B) to determine the association between specific onychoscopic features and the causative organisms.
Participants and methods
This cross-sectional study was done in a tertiary care center in Pondicherry, where all the patients (n = 52) with a clinical diagnosis of onychomycosis attending the dermatology outpatient department in a tertiary care hospital were included. Patients on treatment with topical and systemic antifungals for the past 1 month or patients with other nail diseases, such as traumatic nail dystrophy, nail involvement in lichen planus, and psoriasis, were excluded. The sample size (52) was calculated assuming the prevalence of longitudinal striae and chromonychia on onychoscopy as 84% according to a study done by Abdallah et al.6 with 10% precision and 95% confidence interval. The study was conducted after getting clearance from the research and ethics committees of the institute. (Ref no: IEC: RC/2020/102).
All the patients fulfilling the inclusion criteria were included in the study after obtaining informed consent. A complete history was taken, and a clinical examination was done. Onychoscopic examinations were completed using a Heine MINI 3000 dermoscope, and the findings were documented for all affected fingernails and toenails of each patient. Nail clippings were taken for potassium hydroxide (KOH) mount and fungal culture. When multiple nails were affected, clippings were taken from the most affected nail. KOH mounting was done by keeping a portion of the nail clippings overnight in 20% KOH solution and then examining them using light microscopy (×10 and ×40) for the presence of hyphae, pseudo-hyphae, and yeasts, as described by others7.
Nail clippings were collected from the affected nails under sterile precaution after cleaningwith 70% alcohol on a sterile filter paper. The nails were clipped as proximally as possible from the free edge. he nail clippings were then inoculated into Sabouraud’s dextrose agar containing ccycloheximide. The culture media were incubated at 25°C and 37°C for 4 weeks. Any growth on culture was identified by colony characters and microscopy using Gram’s stain or Lactophenol-cotton blue preparation following the methods described by others8. The phenotypic tests done for the identification of yeasts were the germ tube test, CHROMagar, carbohydrate fermentation, and assimilation test. The molds were identified using Lactophenol cotton blue preparations from slide culture9. After 4 weeks, nail fungal culture reports were noted for each patient.
Data were analyzed using Microsoft Excel software 2017. Quantitative variables were presented in mean, standard deviation, total numbers, and percentages for each category. Student’s t-test and the significance level of p value (p < 0.05) were employed.
Results
The study included 52 patients, 34 females (65.4%), 18 males (34.6%), with ages ranging from 20 years to 67 years (mean 47.2 ± 13 years), mostly between 41 and 50 years of age.
The clinical types identified in this study were, by order of frequency, DLSO (n = 38), TDO (n = 13), and PSO (n = 1). The other clinical types were not observed. The most common nails involved were fingernails, 55.7% (n = 29), compared to toenails, which were 36.5 % (n = 19). 7.8% (n = 5) had both finger and toenail involvement. The clinical examination findings are given in table 1.
Table 1. Results of direct clinical examination
| Findings | Frequency (n) | % |
|---|---|---|
| Nail plate crumbling | 10 | 19.2 |
| Nail plate pitting | 7 | 13.2 |
| Onycholysis | 45 | 86.5 |
| Onychomadesis | 5 | 9.6 |
| Nail dystrophy/Loss of nail plate | 46 | 88.4 |
| Nail bed abnormality | 7 | 13.5 |
| Cuticle absent | 22 | 42.3 |
| Lunula absent | 43 | 82.7 |
| Subungual hyperkeratosis | 15 | 28.8 |
| Chromonychia (discolouration observed in the nail plates) | Frequency (n) | % |
| Yellow, brown | 7 | 13.5 |
| Yellow | 19 | 36.7 |
| Brown | 22 | 42.3 |
| Black | 1 | 1.9 |
| Green | 2 | 3.8 |
| White | 1 | 1.9 |
| Proximal nail fold involvement | 15 | 28.8 |
| Distal nail fold involvement | 10 | 19.2 |
KOH was positive in 32 patients (61.5%), and culture was positive in 35 out of 52 (67.3 %), and both were positive in 21 (40.4%), and both were negative in 6 patients (11.5%) (Table 2). The most common organism found in 18 specimens (34.6%) was Candida spp. (Table 2) which included Candida tropicalis, the commonest species (10 out of 18), Candida albicans, Candida parapsilosis, and Candida guillermondii. Fusarium was cultured in 12 patients, with Fusarium solani as the single 2nd most common organism grown in culture (14%). Other organisms were Cladosporium sphaerospermum, Trichosporon, and Paecillomyces variotti, accounting for 1.9%, 5.8%, and 1.9%, respectively (Table 2). No dermatophytes were found.
Table 2. Potassium hydroxide, culture, and fungus species were identified in the 52 samples collected
| KOH and culture findings | n (%) |
|---|---|
| Results of KOH and nail fungal culture KOH positive Culture positive KOH + culture positive KOH + culture negative | 32 (61.5)35 (67.3)21 (40.4)11 (21.1) |
| Organisms identified in the nail fungal culture Candida tropicalis Candida albicans Candida parapsilosis Candida guilliermondii Fusarium solani Fusarium dimerium Fusarium oxysporum Cladosporium sphaerospermum Trichosporon Paecillomyces variotti No organism growth | 10 (19.2)5 (9.6)1 (1.9)2 (3.8)7 (13.5)1 (1.9)4 (7.7)1 (1.9)3 (5.8)1 (1.9)17 (32.7) |
|
KOH: potassium hydroxide. |
|
The onychoscopic features observed in the nails clinically diagnosed as onychomycosis were mostly chromonychia (n = 52; 100%), particularly a yellow or brown discoloration of the nail plate and onycholysis (n = 52; 100%) (Table 3). Chromonychia was better observed by onychoscopy than through the naked eye, with statistical significance of p < 0.039. The most common color was yellow (32.7%), but many different colors were observed on onychoscopy (Table 3). Onycholysis (Fig. 1A) was also better appreciated by onychoscopy (observed in all patients compared to 50 with naked eye), with distal lateral onycholysis as the topmost feature. The other onychoscopic findings were distal irregular termination (n = 36; 69.2%), rough longitudinal white edge/trachyonychia (n = 32, 61.5%), opacity of the nail plate (n = 31, 59.6%) and longitudinal white striae (n = 31, 59.6%) (Fig. 1B), jagged proximal edge (Fig. 1C) (n = 28; 53.8%) and intermittent spiked pattern (n = 23; 44%). Linear edge (Fig. 1D) as a non-specific feature of onychomycosis was observed in 23.1% patients. Subungual hyperkeratosis (Fig. 1E) observed in 15 patients on clinical examination and 27 on onychoscopy was not significant. A dermatophytoma (Fig. 1F) and fungal melanonychia (Fig. 1G) were observed in 5 patients each (9.6%) and blue-red globules in 2 (3.8%). A “shallow layered appearance” (Fig. 2) was a previously unreported onychoscopic finding observed in 24 patients (46.2%).
Table 3. Onychoscopic features in clinically typical onychomycotic nails
| Onychoscopic features | n (%) |
|---|---|
| Chromonychia (discolouration observed in the nail plates) Yellow, brown Yellow, black Yellow, white Yellow Brownish yellow Brownish black Brown Black Green White Brownish white | 4 (7.7)3 (5.8)2 (3.8)17 (32.9)1 (1.9)5 (9.6)14 (26.9)1 (1.9)2 (3.8)1 (1.9)>2 (3.8) |
| Onycholysis types Distal onycholysis Distal-lateral onycholysis Proximal onycholysis | 11 (21.1)40 (76.9)1 (1.9) |
| Other onychoscopic findings Opacity Longitudinal white striae Jagged proximal edge Intermittent spiked pattern Rough longitudinal white edge/trachyonychia Linear edge Distal irregular termination Subungual hyperkeratosis Dermatophytoma | 31 (59.6)31 (59.6)28 (53.8)23 (44.2)32 (61.5)12 (23.1)36 (69.2)27 (51.9)5 (9.6) |
| Additional onychoscopic findings Fungal melanonychia Blue red globules | 5 (9.6)2 (3.8) |
| Newer onychoscopic findings Shallow-layered appearance | 24 (36.2) |
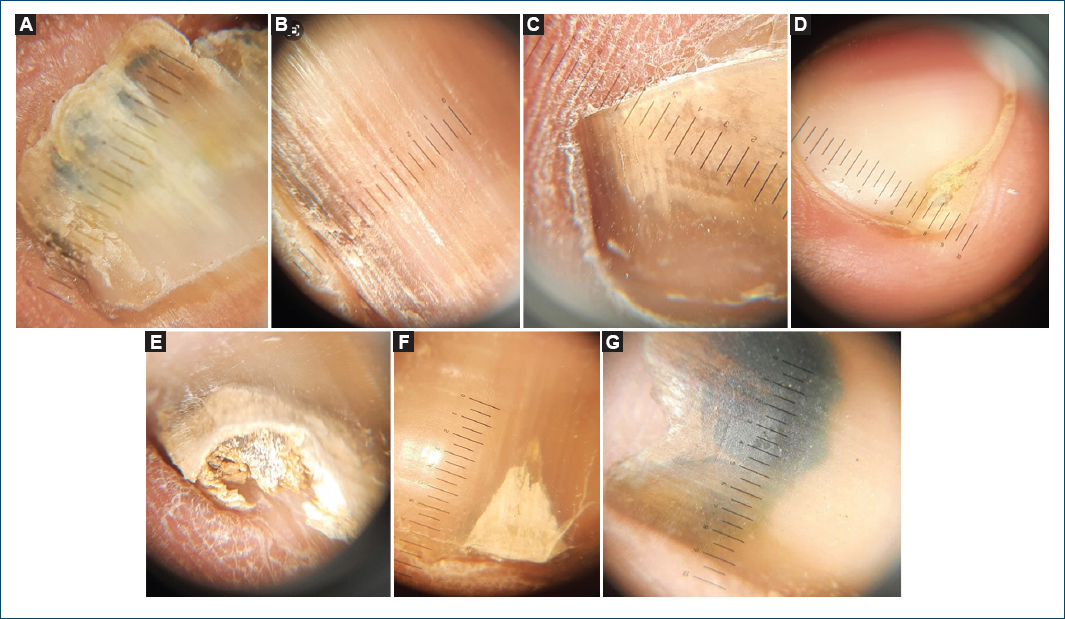
Figure 1. Onychoscopy images. A: onychoscopic image of the affected nail showing onycholysis in the distal and lateral areas of the nail plate seen in candidal onychomycosis. B: onychoscopic image of affected nail showing longitudinal white striae seen in candidal onychomycosis. C: onychoscopic image of affected nail showing jagged proximal edge. D: onychoscopic image of the affected nail showing a linear edge seen in potassium hydroxide (KOH) positive. E: onychoscopic image of affected nail showing subungual hyperkeratosis. F: onychoscopic image of affected nail showing dermatophytoma seen in KOH-positive onychomycosis. G: onychoscopic image of the affected nail showing fungal melanonychia.
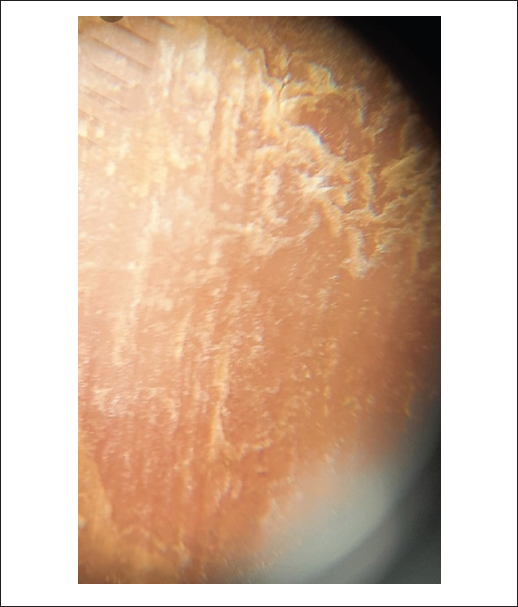
Figure 2. Onychoscopic image of the affected nail showing a shallow layered appearance of the nail plate.
Table 4 shows a comparison of the onychoscopic findings in different cases of onychomycosis (DLSO, TDO, and PSO). The most common color in DLSO was yellow, followed by brown, but other types also showed yellow as the common color. Distal lateral onycholysis was observed in 37 (97.4%) patients with DLSO, which was statistically significant compared to other forms. Subungual hyperkeratosis was significantly less common in DLSO than in other types (p = 0.004). The other findings were non-contributory.
Table 4. Comparison of onychoscopic findings among different types of onychomycosis (DLSO, TDO, and others)
| Onychoscopic findings | Comparison DLSO vs. others | Comparison TDO vs. others | ||||
|---|---|---|---|---|---|---|
| DLSO (n = 38) (%) | Others (n = 14) (%) | p | TDO (n = 13) (%) | Others (n = 39) (%) | p | |
| Chromonychia | 38 | 14 | – | 13 | 39 | – |
| Yellow | 13 (34.2) | 4 (28.6) | – | 4 (30.8) | 13 (33.4) | – |
| Yellowish brown | 4 (10.5) | 2 (14.3) | – | 2 (15.4) | 4 (10.3) | – |
| Yellowish black | 2 (5.3) | 1 (7.1) | – | 1 (9) | 2 (5.1) | – |
| Yellowish white | 2 (5.3) | – | – | – | 2 (5.1) | – |
| Brown | 11 (28.9) | 3 (21.4) | – | 2 (18.2) | 12 (30.8) | – |
| Brownish black | 2 (5.3) | 2 (14.3) | – | 2 (18.2) | 2 (5.1) | – |
| Black | 1 (2.6) | – | – | – | 1 (2.6) | – |
| Green | 2 (5.3) | – | – | – | 2 (5.1) | – |
| White | – | 1 (7.1) | – | 1 (9) | – | – |
| Whitish brown | 1 (2.6) | 1 (7.1) | – | 1 (9) | 1 (2.6) | – |
| Onycholysis | – | – | 0.001 | – | – | 0.001 |
| Distal-lateral | 37 (97.4) | 3 (21.4) | – | 3 (23.1) | 37 (94.8) | – |
| Total nail | – | 10 (71.4) | – | 10 | – | – |
| Proximal | – | 1 (7.1) | – | – | 1 (2.6) | – |
| Opacity | 23 (60.5) | 8 (57.1) | 1.000 | 7 (53.8) | 24 (61.5) | 0.747 |
| Longitudinal white striae | 21 (55.3) | 10 (71.4) | 0.353 | 9 (69.2) | 22 (56.4) | 0.523 |
| Jagged proximal edge | 21 (55.3) | 7 (50) | 0.764 | 6 (54.5) | 22 (56.4) | 0.541 |
| Intermittent spiked pattern | 16 (42.2) | 7 (50) | 0.755 | 6 (46.1) | 17 (43.6) | 1.000 |
| Rough longitudinal white edge/trachyonychia | 21 (55.3) | 11 (78.6) | 0.200 | 10 (76.9) | 22 (56.4) | 0.324 |
| Linear edge | 10 (26.3) | 2 (14.3) | 0.475 | 2 (18.2) | 10 (25.6) | 0.706 |
| Distal irregular termination | 24 (63.2) | 12 (85.7) | 0.179 | 11 (84.6) | 25 (64.1) | 0.298 |
| Subungual hyperkeratosis | 15 (39.5) | 12 (85.7) | 0.004 | 11 (84.6) | 15(38.5) | 0.010 |
|
DLSO: distal lateral subungual onychomycosis; TDO: total dystrophic onychomycosis. |
||||||
Subungual hyperkeratosis, observed in 11 out of 13 of TDO cases (84.6%), was significantly more frequent in this type compared to others (p = 0.010). Longitudinal white striae, intermittent spiked pattern, rough longitudinal white striae, and distal irregular termination were more frequent in TDO, but with no statistically significant difference. The only patient with PSO presented with brown discoloration, proximal onycholysis, and opacity of the nail plate, jagged proximal edge, intermittent spiked pattern, and distal irregular termination.
When comparing the onychoscopic features of onychomycosis caused by Candida with others, there was no remarkable difference in colour (Table 5), but distal irregular termination was significantly lower (50% vs. 79.4%), and a linear edge, observed in 88% of candidal onychomycosis, and subungual hyperkeratosis observed in 38.8% were not significantly different.
Table 5. Comparison of the onychoscopic findings among organisms of culture
| Onychoscopic findings | Comparison Candida vs. others | Comparison Fusarium vs. others | ||||
|---|---|---|---|---|---|---|
| Candida (n = 18) (%) | Others (n = 34) (%) | p | Fusarium (n = 12) (%) | Others (n = 4) (%) | p | |
| Chromonychia | – | – | – | – | – | – |
| Yellow | 8 (44) | 9 (26.5) | – | 3 (25) | 14 (35) | – |
| Yellowish brown | 2 (11) | 3 (8.8) | – | 1 (8.3) | 4 (10) | – |
| Yellowish black | 1 (5.5) | 2 (5.9) | – | 1 (8.3) | 2 (5) | – |
| Yellowish white | – | 2 (5.9) | – | 1 (8.3) | 1 (2.5) | – |
| Brown | 5 (27.5) | 9 (26.5) | – | 4 (33.3) | 10 (25) | – |
| Brownish black | 2 (11) | 3 (8.8) | – | 1 (8.3) | 4 (10) | – |
| Black | – | 1 (2.9) | – | 1 (8.3) | – | – |
| Green | – | 2 (5.9) | – | – | 2 (5) | – |
| White | – | 1 (2.9) | – | – | 1 (2.5) | – |
| Whitish brown | – | 2 (5.9) | – | – | 2 (5) | – |
| Onycholysis | – | – | – | – | – | – |
| Distal-lateral | 13 (72.2) | 27 (79.4) | 0.505 | 9 (75) | 31 (77.5) | 0.466 |
| Total nail | 4 (22.2) | 7 (20.6) | – | 2 (16.6) | 8 (20) | – |
| Proximal | – | – | – | – | – | – |
| Opacity | 11 (61.1) | 20 (58.8) | 1.000 | 6 (50) | 25 (80) | 0.512 |
| Longitudinal white striae | 8 (44.4) | 23 (67.6) | 0.141 | 6 (50) | 25 (80) | 0.512 |
| Jagged proximal edge | 6 (33.3) | 22 (64.7) | 0.043 | 10 (83.3) | 18 (40) | 0.024 |
| Intermittent spiked pattern | 9 (50) | 14 (41.2) | 0.571 | 8 (66.6) | 15 (37.5) | 0.102 |
| Rough longitudinal white edge/trachyonychia | 11 (61.1) | 21 (61.8) | 1.000 | 7 (58.3) | 25 (20) | 1.000 |
| Linear edge | 6 (33.3) | 6 (17.6) | 0.300 | 3 (25) | 9 (40) | 1.000 |
| Distal irregular termination | 9 (50) | 27 (79.4) | 0.056 | 9 (75) | 27 (60) | 0.733 |
| Subungual hyperkeratosis | 7 (38.8) | 20 (58.8) | 0.245 | 6 (50) | 21 (40) | 1.000 |
Fusarium-affected nails showed more brown discolorations (33.3%), but less nail plate opacity (50% vs. 80%). Jagged proximal edges, distal irregular termination, intermittent spiked pattern, and rough longitudinal white edge were very frequently observed in these affected nails (Table 5).
In three patients with Trichosporon infection, all with DLSO, two showed yellow and one green colour, all had longitudinal striae and distal irregular termination, two had opacity and jagged proximal edge, and one had trachyonychia.
Discussion
Our study was carried out in 52 adult patients with onychomycosis within the most common age group (40-50 y), with more females, similar to other reported studies10,11. DLSO was the commonest type of clinical presentation in all organisms, namely in Candida, Fusarium, and Trichosporon infections. The only case of PSO showed Candida on culture, and Candida spp was also the most common isolate in TDO.
Comparing onychoscopic features of our studies with previous ones (Table 6)4,11–14. We found a previously unreported finding in 46.2% of onychomycosis, a “shallow layered appearance.”
Table 6. Comparison of onychoscopic findings with previous studies4,11–14
| Study | Sample size | Distal irregular termination (%) | Longitudinal striae (%) | Intermittent spiked pattern (%) | Chromonychia (%) | Subungual hyperkeratosis (%) |
|---|---|---|---|---|---|---|
| Jesus-Silva et al. | 155 | 43.23 | 60.7 | 25 | 21.94 | – |
| Maatouk et al. | 45 (DLSO) | 5-11 | 31-68 | 25-55 | – | – |
| Chetana et al. | 234 | 34.6 | 49.1 | 43.6 | – | – |
| Kayarkatte et al. | 88 | 81.8 | 25 | 86.4 | 85.2 | 85.2 |
| Sangeetha et al. | 122 | 23 | 81.1 | 80.3 | – | – |
| Our study | 52 | 69.2 | 59.6 | 44.2 | 100 | 51.9 |
In our study, most patients with DLSO presented with yellowish discoloration, distal lateral onycholysis, distal irregular termination, and nail plate opacity (60.5%) but only 55.3% of DLSO showed longitudinal white striae, in contrast to studies done by Jesus-Silva et al. (62.6%), Nargis et al. (100%), (100%), and Yadav et al. (100%)4,15,16 TDO type presented with total nail onycholysis, distal irregular termination, and subungual hyperkeratosis (81.8%), similar to the study by Chetana et al., but longitudinal white striae were much more frequent in our study (63.3% vs. 10%)12.
The association between clinical features, onychoscopic findings, and etiology based on nail culture has rarely been studied. In our study, nails with candidal growth in culture showed more common yellow and brown discolouration compared to other organisms, whereas nail plate opacity, intermittent spiked pattern, and linear edge were only slightly more frequent. Compared to the study by Abdallah et al.6 that found mostly longitudinal white striae (85.7%), spiked pattern (64%), subungual hyperkeratosis (42%), distal irregular termination (57.7%), and jagged proximal edge (64%) in candidal nail infection, our findings are not significantly different.
We cannot compare our results in onychomycosis due to Fusarium or due to Trichosporon because, as far as we know, there are no published studies on onychoscopic findings in the nail infections by these agents.
Limitations
The small study population is a limitation. The diagnostic accuracy of onychomycosis could have been augmented if histopathological examination and Periodic Acid-Schiff stain were used. The low culture positivity rate and absence of dermatophytes in culture limit the generalization of this study.
Conclusions
Onychoscopy can be used as a non-invasive diagnostic aid in onychomycosis, where investigations such as KOH examination and culture have low sensitivity. Chromonychia and onycholysis are observed on onychoscopy in almost all patients. Shallow-layered appearance is a newly detected onychoscopic feature, whose specificity needs to be evaluated. Distal irregular termination was significantly lower in candidal onychomycosis compared to others. Fusarium-affected nails showed more brown discolorations and jagged proximal edges and an intermittent spiked pattern in onychoscopy than others. This study shows an association between onychoscopic features and the causative agents in onychomycosis, but further studies with a substantial use of onychoscopy are necessary for defining the real value of onychoscopy in diagnosing onychomycosis and suggesting its cause, therefore contributing to better orient its treatment.
Funding
None.
Conflicts of interest
None.
Ethical considerations
Protection of human subjects and animals. The authors declare that the procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation and with the World Medical Association and the Declaration of Helsinki. The procedures were authorized by the Institutional Ethics Committee.
Confidentiality, informed consent, and ethical approval. The authors have followed their institution’s confidentiality protocols, obtained informed consent from all patients, and secured approval from the Ethics Committee. SAGER guidelines have been followed as applicable to the nature of the study.
Declaration on the use of artificial intelligence (AI). The authors declare that no generative artificial intelligence was used in the writing or creation of the content of this manuscript.
