We present the case of a 56-year-old woman with a congenital yellowish lesion on her scalp that had remained stable until approximately 18 months before evaluation. During this period, she noted the appearance of new growths on the lesion, which exhibited progressive enlargement and occasional spontaneous bleeding. On physical examination, a sessile, yellow-brown, verrucous plaque with well-defined, irregular borders, measuring approximately 4 × 1.5 cm, was observed on the interparietal scalp (Fig. 1). At the anterior margin of the plaque, a violaceous nodule with macroscopic telangiectasias, measuring approximately 1.5 cm in its greatest dimension, was identified (Fig. 1). Posterior to this, an 8-mm violaceous papule with similar features was noted (Fig. 1). Dermoscopy revealed telangiectasias and a bluish coloration (Fig. 2). Surgical excision of both lesions was performed, and histopathological examination confirmed basal cell carcinoma (BCC) arising within a nevus sebaceous, with clear surgical margins.

Figure 1. Physical examination showing a sessile, yellow-brown, verrucous plaque with well-defined, irregular borders, measuring approximately 4 × 1.5 cm on the scalp. Anteriorly, a violaceous nodule with macroscopic telangiectasias measures approximately 1.5 cm at its greatest dimension, and posteriorly, an 8-mm violaceous papule is present.
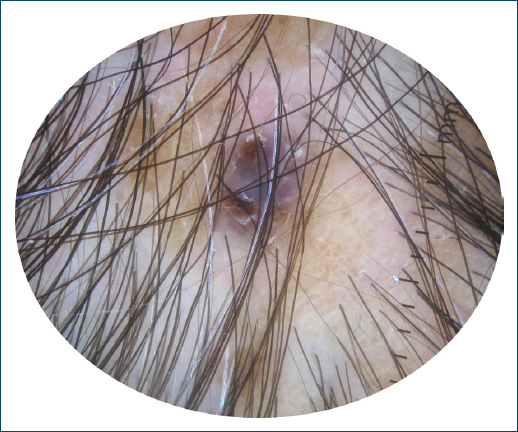
Figure 2. Dermoscopy reveals peripheral telangiectasias and a bluish coloration.
Nevus sebaceous, also known as nevus sebaceous of Jadassohn, is a hamartomatous lesion originating from follicular, sebaceous, apocrine, and connective tissue components1,2. These lesions typically present at birth or in early childhood, often as yellow to orange patches or plaques with associated alopecia1. While the scalp is the most common site, nevus sebaceous can also occur on the face, neck, and other regions1. Although predominantly congenital, sporadic cases have been documented, sometimes associated with genetic syndromes, such as Schimmelpenning-Feuerstein-Mims syndrome1.
The clinical morphology of nevus sebaceous evolves with age. In childhood, the lesion is generally stable, appearing as a smooth or slightly raised patch1. Hormonal changes during puberty often lead to thickening and a more verrucous appearance1. Significant morphological changes, such as rapid growth, ulceration, or spontaneous bleeding, should prompt further evaluation, including biopsy, to exclude malignant transformation.
Nevus sebaceous carries a lifetime risk of secondary neoplasms, estimated at 10-20%2. Most secondary neoplasms are benign and of follicular origin3, such as trichoblastomas or sebaceomas. Malignant transformation is rare, occurring in < 1% of cases, with BCC being the most commonly reported malignancy, followed by squamous cell carcinoma and sebaceous carcinoma1. When malignant neoplasms develop, they typically present in adulthood2, as demonstrated in this case.
Histopathological confirmation of BCC arising within a nevus sebaceous is essential for guiding appropriate treatment. Surgical excision with histologically confirmed clear margins is the preferred management approach. Complete excision minimizes the risk of recurrence and allows for histopathological assessment of the entire lesion to rule out additional neoplastic changes. Clinical follow-up is recommended to monitor for recurrence or the emergence of new neoplasms.
This case emphasizes the importance of vigilance in monitoring nevus sebaceous for signs of malignant transformation. The development of new nodules, spontaneous bleeding, or ulceration should prompt immediate evaluation and intervention. Early detection and management of neoplastic transformation are critical to improving patient outcomes. Our case highlights the necessity of clinical and histopathological correlation in managing nevus sebaceous and emphasizes the importance of regular follow-up for these patients.
Author contributions
M. Mendes-de Carvalho: manuscript preparation and elaboration. L. Silva: acquisition of clinical images and critical review of the manuscript.
Funding
None.
Conflicts of interest
None.
Ethical considerations
Protection of human subjects and animals. The authors declare that no experiments on humans or animals were performed for this research.
Confidentiality, informed consent, and ethical approval. The authors have followed their institution’s confidentiality protocols, obtained informed consent from all patients, and secured approval from the Ethics Committee. SAGER guidelines have been followed as applicable to the nature of the study.
Declaration on the use of artificial intelligence (AI). The authors declare that no generative artificial intelligence was used in the writing or creation of the content of this manuscript.
