Introduction
Desmoplastic trichoepithelioma (DT) is a rare benign skin neoplasm of the hair follicle, a variant of trichoblastoma originating from the proliferation of mesenchymal cells1–3. The classification of this cutaneous neoplasm can be divided into three forms: familial multiple trichoepithelioma, solitary, and desmoplastic, with the desmoplastic form characterized by increased fibroplasia in the dermis and this tumor should be considered a differential diagnosis for basal cell carcinoma (BCC)1–3.
In addition, DT shows a predilection for females, particularly young or middle-aged women4,5. Its most common manifestations occur on the facial skin as pink or skin-colored papules and nodules that progressively increase in size, often easily confused with the clinical aspects of BCC4,5. The histopathology of this neoplasm consists of a histological triad of thin cords of basaloid cells, keratin cysts, and desmoplastic stroma, which are important for both histological differential diagnoses and clinical differentiation from BCC3–7.
Case report
A 54-year-old female patient was referred for a dermatological consultation due to a facial lesion that had been present for approximately 2 years, showing progressive growth over time without associated symptoms (Fig. 1).
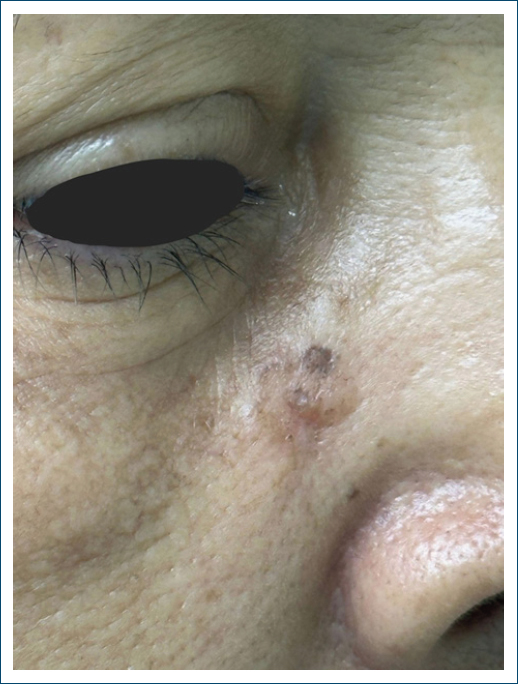
Figure 1. Clinical appearance of the neoplasm.
On dermatological examination, a brownish plaque with some black-pigmented areas, irregular shape, pearly shine, and telangiectasias on its surface was observed, measuring 1 cm in the right paranasal region (Fig. 2).
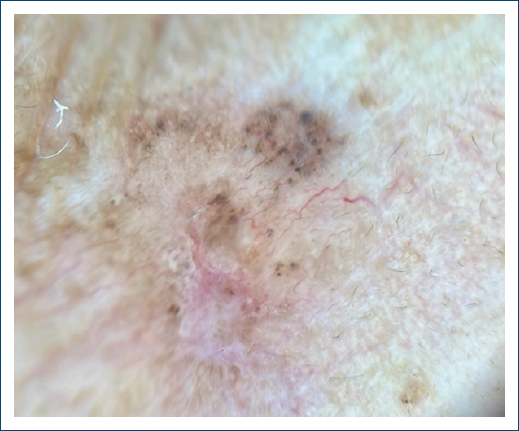
Figure 2. Dermatoscopy of the lesion with irregularly distributed black pigment, tortuous vessels, and mild erythema, measuring 1 cm.
The patient underwent an incisional biopsy of the lesion, followed by histopathological examination, which showed atrophic epidermis and dermis with diffuse proliferation of small nodular masses and cords of basaloid cells with peripheral palisading, including occasional horn cysts, embedded in desmoplastic and myxoid stroma. Bulb-papilla images suggested follicular differentiation (Fig. 3).
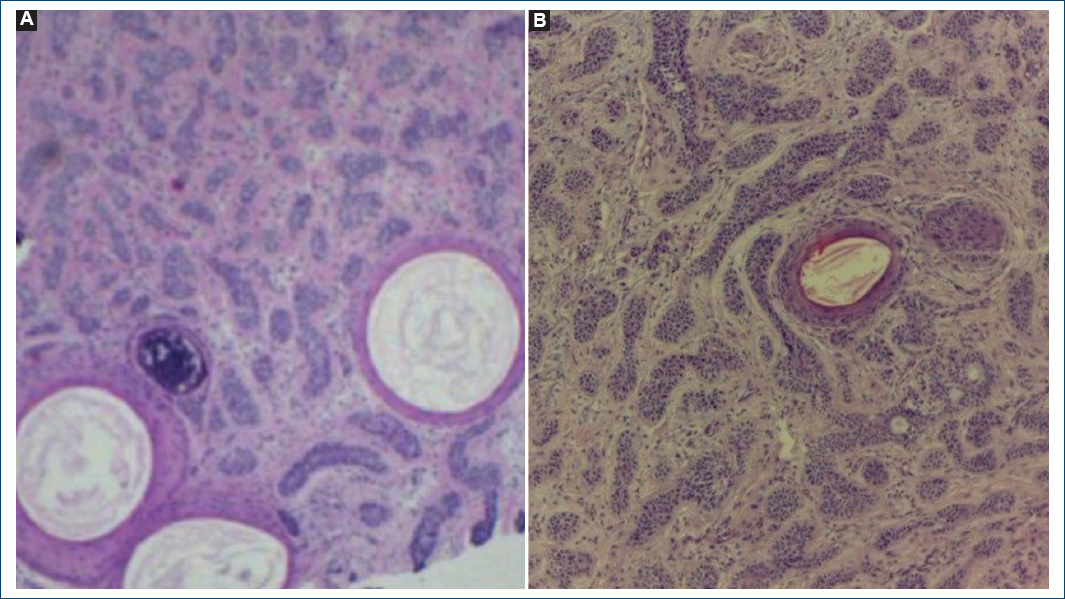
Figure 3. Histopathological findings. A and B: histological sections, horn cysts, embedded in desmoplastic and myxoid stroma (H&E, x40).
The histopathological examination revealed an intradermal epithelial neoplasm, raising differential diagnoses of DT, micronodular BCC, and microcystic adnexal neoplasm. An additional immunohistochemical study confirmed the diagnosis of DT (Table 1).
Table 1. Results of the immunohistochemical panel
| Antibody | Clone | Result | Observation |
|---|---|---|---|
| Ki-67 (cell proliferation antigen) | MIB1 | Positive | 5% |
| p63 protein (squamous/transitional epithelia; myoepithelial cells) | DAK-p63 | Positive | – |
| Epithelial tumor glycoprotein | BerEp4 | Positive | – |
| Epithelial membrane antigen | E29 | Negative | – |
| Anti-apoptotic protein BCL-2 | 124 | Negative | – |
Following the DT diagnosis, clinical follow-up of the patient was chosen.
Discussion
BCC is the most common skin neoplasm among non-melanoma skin cancers. Histopathological classification divides BCC into types such as nodular, superficial, and infiltrative. Despite its rare metastatic potential, BCC significantly impacts patient morbidity1–3. DT is a benign cutaneous tumor that differentiates into germinative hair follicle cells1–3. Representing < 1% of all skin tumors, its clinical and histopathological similarities with BCC components pose a controversy in both dermatologic surgery and clinical settings, as this neoplasm has a rare chance of malignant transformation3–7.
According to Rezze et al. dermoscopy is an essential technique in the clinical approach to skin lesions, playing a key role in identifying malignant lesions such as BCC8. However, dermoscopic findings in DT can mimic BCC structures, such as pearly shine and branching telangiectasias9. While arborizing telangiectasias are common in many cutaneous neoplasms, these vessels are thicker and more branched in nodular BCC, unlike the finer, less branched vessels in DT, which aligns with this patient’s dermoscopic findings9.
Histopathological findings in trichoepithelioma are characterized by basaloid cell proliferation, compact desmoplastic stroma, small cysts lined with keratinized epithelium, and sometimes calcifications. These features overlap with BCC, necessitating immunohistochemical studies for definitive diagnosis, as trichoepithelioma does not express carcinoembryonic antigen10–14.
Studies like Bains et al. used markers CK20, Ki-67, Bcl-2, CD10, and CD34 in immunohistochemistry to evaluate reactivity between the two neoplasms discussed. However, CD34, CD10, and CK20 markers were not used in this case; only Bcl-2 and Ki-67 were applied15. The Ki-67 marker showed 5-10% tumor cell proliferation, consistent with Bains et al.’s findings, while Bcl-2 did not show reactivity, highlighting the need to define an immunohistochemical panel to differentiate this benign tumor from other malignant neoplasms15.
Given this, there is limited scientific evidence on trichoepithelioma and its variants, especially the desmoplastic form, as it is a rare neoplasm with low population incidence. Only one publication exists in Brazilian literature. Furthermore, few studies address specific markers for identifying and differentiating this disease. Thus, continuous monitoring of suspected DT lesions is crucial to correctly rule out malignant cutaneous diagnoses and implement appropriate therapeutic management.
Conclusion
The patient in this case report presents with DT, a rare but benign tumor that clinically and histopathologically resembles BCC. Immunohistochemistry is an essential and necessary test for diagnostic confirmation and for defining the appropriate therapeutic management. In addition, there is limited literature evaluating the desmoplastic form of trichoepithelioma and its histological or immunohistochemical diagnosis. Therefore, careful attention is needed to avoid diagnostic errors and unnecessary treatments for patients diagnosed with this condition.
Funding
None.
Conflicts of interest
None.
Ethical considerations
Protection of human subjects and animals. The authors declare that no experiments on humans or animals were performed for this research.
Confidentiality, informed consent, and ethical approval. The authors have followed their institution’s confidentiality protocols, obtained informed consent from all patients, and secured approval from the Ethics Committee. SAGER guidelines have been followed as applicable to the nature of the study.
Declaration on the use of artificial intelligence (AI). The authors declare that no generative artificial intelligence was used in the writing or creation of the content of this manuscript.
