Introduction
Eccrine spiradenoma is a rare benign adnexal tumor first described in 1956 by Kersting and Helwig as a dermal tumor with sweat gland differentiation1. Recent immunohistochemical studies using follicular stem cell markers (e.g., CD200) have suggested a possible origin in the hair follicle bulge, placing it closer to the folliculosebaceous-apocrine unit2.
Spiradenomas usually occur in patients between 15 and 35 years old, and there is no racial or sexual predilection for them3. They typically present as strikingly painful small solitary nodules on the head, neck, and trunk that can grow to several centimeters, often with a blue, gray, or purple hue3,4.
Spiradenomas appear to be caused by a defective tumor suppressor gene5. While a mutation in the CYLD gene on chromosome 16 is found in Brooke-Spiegler syndrome, which features multiple spiradenomas, the specific cause of solitary spiradenomas is not clear5.
Although benign spiradenomas are rare, malignant transformation is even rarer and occurs almost exclusively in patients older than the age of 50 years6,7.
This three-case series provides illustrative examples of the histological diversity and diagnostic complexity of eccrine spiradenomas.
Case report
Case 1
A 62-year-old male patient with an unremarkable previous medical history sought treatment for a painless lesion on the right arm that he had for, at least, 2 years. On examination, a 1.5 × 1.3 cm erythematous and nodular lesion was found. Figures 1 A and B illustrates the histopathological findings.
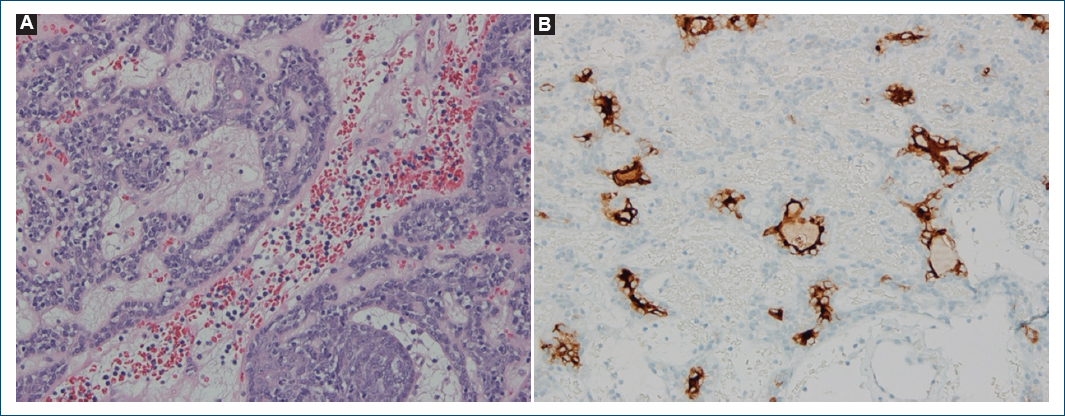
Figure 1. Histopathological findings. A: tumor composed of nests and cords of cells surrounded by basement membrane material and composed of two types of cells (clear and dark cells) with some ductal structures (H&E, ×200); B: luminal cells of ductal structures with immunoreactivity for EMA (EMA, ×400).
Case 2
A 38-year-old male patient with no previous medical history sought treatment for a painless lesion in the lower anterior right hemithorax that he had for many years. On examination, a 0.9 × 0.7 cm nodular lesion was found. Figures 2 A–C illustrates the histopathological findings.
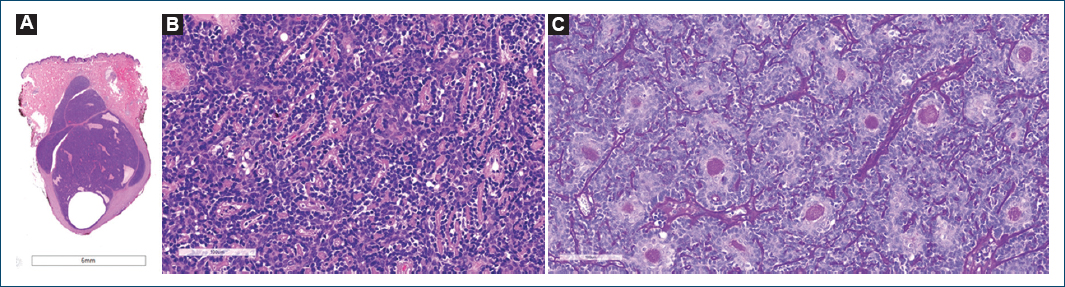
Figure 2. Histopathological findings. A: dermis and hypodermis exhibit a well-circumscribed nodular basophilic tumor with cystic changes (H&E, low magnification); B: tumor is composed of dual cell population arranged in trabecular fashion with tubular structures (H&E, ×200); C: PAS stains basement membrane material within the tubules (PAS, ×200).
Case 3
A 58-year-old male patient with no previous medical history sought treatment for a painful lesion on the right forearm that he had for 1 year. On examination, a 1.0 × 0.9 cm superficial and mobile nodule was found. Figures 3 A–D illustrates the histopathological findings.
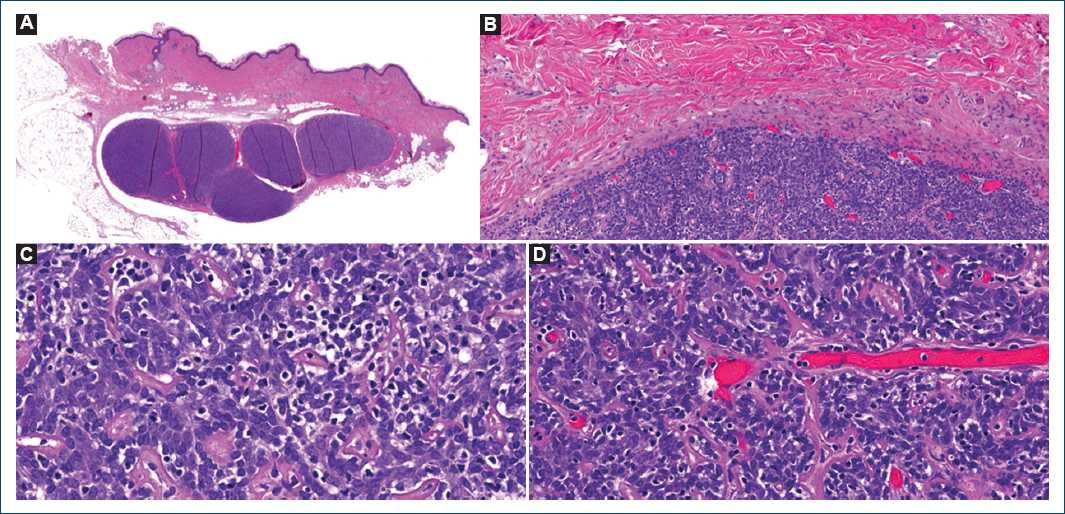
Figure 3. Histopathological findings. A: well-circumscribed, basophilic tumor lobules in the dermis and subcutaneous tissue (H&E, low magnification); B: the tumor lobules are well marginated and encapsulated by a thin fibrous capsule (H&E, ×100); C: the tumor is composed of a biphasic population of smaller basaloid cells and larger clear cells. There is no cytologic atypia, mitosis, or necrosis (H&E, ×200); D: vascular stroma with capillary ectasias, basement membrane material, and scattered lymphocytes (H&E, ×200).
HISTOLOGICAL DESCRIPTION
Histological examination of all three cases revealed a well-defined, encapsulated neoplasm located in the dermis and extending into the subcutaneous tissue. The tumors exhibited a dual cell population, with centrally located large, pale cells containing moderate cytoplasm and vesicular nuclei, and peripheral small, basaloid cells with scant cytoplasm and hyperchromatic nuclei. The lobules were surrounded by basement membrane-like material, which was PAS positive. The stroma was vascularized and populated by numerous lymphocytes, with vascular ectasias also noted in some cases. No cytological atypia, mitosis, or necrosis was observed in any of the lesions. Surgical margins were free of tumor in all cases. In addition, in Case 1, lymphoid inflammatory infiltrates and vascular ectasias and EMA expression in neoplastic epithelial cells were also described.
Discussion
The three cases presented highlight both the similarities and variations in the clinical presentation, histopathological findings, and diagnostic considerations of eccrine spiradenomas.
Although typically reported in younger patients, without sexual predilection, this series highlights eccrine spiradenomas in older males (38-62 years), suggesting either a skewed demographic or an underreported trend.
The location of the tumors in these cases varied, with two cases presenting in the upper limbs (right arm and right forearm) and one on the right hemithorax. This is consistent with the literature indicating a predilection for the ventral surface of the upper half of the body8.
The main clinical feature, present in about 91% of the patients, is the presence of paroxysmal pain or sensitivity1. However, only one of the three patients (Case 3) reported pain. The absence of pain in the other two cases highlights the variability of symptomatology, even in tumors classically described as painful.
In all cases, the lesions were initially suspected to be other cutaneous conditions – such as hemangioma, epidermoid cyst, lipoma, dermatofibroma, neurofibroma, leiomyoma, schwannoma, and nodular basal cell carcinoma – underscoring the clinical challenge of diagnosing eccrine spiradenomas based on clinical features alone. Notably, several of these entities also fall within the differential diagnosis of painful skin tumors, often remembered through the mnemonic “LEND AN EGG,” which includes leiomyoma, eccrine spiradenoma, neuroma, dermatofibroma, angiolipoma, neurilemmoma, endometrioma, glomus tumor, and granular cell tumor9. This further reinforces the necessity of histopathological examination for accurate diagnosis, which remains the gold standard.
Although most spiradenomas are sporadic and solitary, a subset may arise in the context of Brooke-Spiegler syndrome (also known as CYLD cutaneous syndrome), an autosomal-dominant disorder characterized by multiple benign adnexal tumors, most commonly spiradenomas, cylindromas, and trichoepitheliomas that typically manifest during childhood or early adolescence10–12. None of the patients had a personal history of excision of other benign cutaneous tumors nor any family history suggestive of Brooke-Spiegler syndrome. On physical examination, the tumors appeared to be isolated lesions without other adnexal tumors, and none had arisen during childhood or adolescence. In addition, during a one-year follow-up period, no new benign skin tumors were identified. Therefore, although clinical genetic testing for a germline CYLD pathogenic variant should be considered in individuals with two or more biopsy-confirmed cylindromas, spiradenomas, or trichoepitheliomas, alone or in combination, such testing was not deemed necessary in these cases.
Conclusion
This series of three cases reinforces the clinical and histopathological diversity of eccrine spiradenomas, while also challenging conventional assumptions regarding their demographic and anatomical distribution. The presentation in older male patients, with predominantly painless lesions and locations on the ventral upper body, highlights the need to consider this diagnosis even in atypical contexts. The histological findings further illustrate the spectrum of morphological variability. Moreover, the absence of features suggestive of CYLD cutaneous syndrome emphasizes the importance of clinical evaluation in determining the need for genetic testing. Ultimately, this series underscores the diagnostic value of histopathology in distinguishing eccrine spiradenomas from other painful or indolent subcutaneous tumors.
Funding
None.
Conflicts of interest
None.
Ethical considerations
Protection of human subjects and animals. The authors declare that no experiments on humans or animals were performed for this research.
Confidentiality, informed consent, and ethical approval. The authors have obtained approval from the Ethics Committee for the analysis of routinely collected and anonymized clinical data; therefore, individual informed consent was not required. Relevant ethical recommendations have been followed.
Declaration on the use of artificial intelligence (AI). The authors declare that no generative artificial intelligence was used in the writing or creation of the content of this manuscript.
