Introduction
Psoriasis is a chronic, immune-mediated inflammatory disease characterized by erythematous, scaly, infiltrated, and pruritic plaques on the skin. It typically affects the extensor surfaces, scalp, palms, soles, and nails; however, it can involve any area of the integument. It has a negative impact on the quality of life of affected patients and can be associated with comorbidities such as psoriatic arthritis.1
Genital psoriasis usually presents as erythematous, well-defined plaques with varying degrees of desquamation. Symptoms such as pruritus, burning, and dyspareunia have been reported.2 Therefore, genital psoriasis can significantly affect the quality of life, psychological well-being, and sexual health of affected patients.3
In Brazil, the estimated prevalence of psoriasis ranges from 1.2% to 2.5%.4,5 However, genital involvement is not widely described. It is estimated that genital involvement occurs in more than two-thirds of patients;6 however, this proportion may be underestimated, as these areas may not be actively questioned or assessed during the clinical examination.7
This paper aims to explore clinical aspects of genital psoriasis, including its prevalence, impact on sexual health and treatment options.
Epidemiology
Among the various dermatoses that can affect the genitals, psoriasis is the most common.8 A systematic review conducted by Meeuwis et al., including 18 studies and a total of 22.116 patients with psoriasis, showed that approximately 63% of patients will present some genital involvement during the course of the disease. This proportion increases to 79% when the patient has the flexural or inverted clinical form of the disease.6
In a prospective study totaling 776 patients with psoriasis, 43.2% of the patients had genital involvement.2 An Indian study examining 852 patients with psoriasis reported a lower prevalence of 11.7%.9 A prospective observational study with a total of 262 patients, 42% Chinese, 36.6% Malay and 21.4% Indian or other nationalities, showed 46.1% genital involvement by psoriasis currently or previously to the study.7 Curiously, this study also identified that being Chinese was a risk factor for genital psoriasis when compared to the other ethnicities included.7
Men are more frequently affected by genital psoriasis than women6,7,10 and it manifests simultaneously with lesions on other parts of the body in the majority of cases, with isolated genital involvement being reported in only 2-5% of cases.11 More severe cases, as assessed by the psoriasis area and severity index (PASI), and the greater use of systemic therapies have been associated with genital psoriasis.2 A Swiss study evaluated 109 children with psoriasis, and genital involvement was present in around 40% of them and was often the first manifestation of the disease.12 Circumcision apparently does not influence the development of genital psoriasis in men.2
Clinical manifestations
The most characteristic lesions are well-defined erythematous plaques with minimal infiltration. Unlike lesions in other regions of the body, desquamation may be absent, possibly due to increased local humidity and friction.13 However, typical scales may be present in more keratinized areas (Fig. 1).14 The areas mostly affected in men include the body of the penis, the scrotum, and, less commonly, the glans (Fig. 2). In women, the labia majora are the most commonly affected areas and are often symmetrically involved, followed by the perineum.2

Figure 1. Erythematous and scaly plaques affecting the base of the penis and the pubic region of a male patient with psoriasis.

Figure 2. Erythematous plaques affecting the dorsal region of the penile body in a male patient with psoriasis.
Pruritus is the main symptom of genital psoriasis, reported by more than 86% of patients; however, around half of the cases experience pain, burning, and discomfort during sexual intercourse due to the presence of fissures.2 Due to the Koebner phenomenon, genital psoriasis can be aggravated by irritation caused by urine and feces, tight clothing, and trauma from sexual intercourse.15
Genital psoriasis is not a static disease; in general, its worsening occurs in parallel with the progression of non-genital lesions, although there are exceptions.16 The main worsening factors traditionally described include emotional stress, trauma, some medications, and friction (related to sexual activity or wearing tight clothing).3 Studies show that up to 34% of patients experience post-coital worsening.2,17
The diagnosis of genital psoriasis is essentially clinical, and biopsy is avoided in these cases due to the sensitivity of the area. Therefore, as a non-invasive method, dermoscopy may serve as an additional diagnostic tool. Dotted vessels and dilated, tortuous capillaries distributed over a homogeneous reddish background represent the most frequently described pattern.18
Psoriasis is a condition that generally does not lead to tissue fibrosis; however, Albert et al. described two cases of female patients with long-term genital psoriasis who developed fibrosis and loss of the labia minora.19 Secondary infection by bacteria, fungi, or viruses is relatively common and can aggravate symptoms or cause atypical manifestations. Therefore, in the event of clinical suspicion, the infection should be treated promptly.13 A retrospective observational study showed that more than a third of patients with genital psoriasis had positive swabs for Candida albicans or Staphylococcus spp.20
Differential diagnoses
The differential diagnosis of genital psoriasis encompasses a broad spectrum of inflammatory and infectious dermatoses, including candidiasis, contact dermatitis, lichen planus, lichen sclerosus, and sexually transmitted infections, all of which may exhibit overlapping clinical features in the genital region.11,21 Genital psoriasis may pose a significant diagnostic challenge, particularly when lesions are isolated and not accompanied by extragenital manifestations.11,22 In such circumstances, clinical overlap with premalignant and malignant conditions must be considered. Squamous cell carcinoma, including erythroplasia of Queyrat, may closely mimic genital or inverse psoriasis, potentially leading to diagnostic misinterpretation and delayed treatment.23 Although the diagnosis of genital psoriasis is typically clinical, current evidence supports a low threshold for performing a skin biopsy in cases of solitary, persistent, atypical, or treatment-refractory genital lesions, to exclude malignancy and ensure diagnostic accuracy.11,22,23
Severity assessment tools
The assessment tools traditionally used in psoriasis may not be suitable for the genital form of the disease. The PASI and body surface area are tools that depend on the area of the affected body surface, so in genital psoriasis alone, they will not be able to demonstrate the severity of the disease adequately.24 Although the dermatology life quality indexincludes, in item 9, the impact of the disease on sexual life, it is not specific to genital psoriasis.25 Therefore, more specific tools have been developed in order to refine this assessment, including the genital psoriasis sexual frequency questionnaire and the genital psoriasis symptoms scale.26
Treatment
The treatment of genital psoriasis is challenging due to the particularities of the skin in this area. Patients should be informed that the disease is neither transmissible nor the result of poor hygiene. In addition, teaching them to use non-irritating cleansers, topical medication in sufficient quantities, and moisturizing the area helps with the therapeutic response. Furthermore, the use of intimate lubricants during sexual intercourse reduces friction and, consequently, the risk of Koebner’s phenomenon.27
Therapy with topical corticosteroids, alone or in combination with systemic drugs, has been shown to be the initial treatment of choice for genital psoriasis.28 As the skin is thinner and subject to natural occlusion, percutaneous absorption is increased;29 therefore, the use of low-potency topical corticosteroids, such as hydrocortisone, is recommended, and their effectiveness has been demonstrated in prospective and retrospective studies.6,20,30,31 It is recommended not to extrapolate the use time of four continuous weeks to minimize the risk of well-known adverse events, including skin atrophy, telangiectasias, and stretch marks.28
Although low or medium potency corticosteroids are preferable for sensitive areas such as the genitals, high potency corticosteroids may be indicated for short periods in moderate to severe cases or to induce an initial clinical response.20 Formulations with Vitamin D analogues, such as calcipotriol, can be used in conjunction with corticosteroids or even after their use.31
Topical calcineurin inhibitors (TCI), such as tacrolimus and pimecrolimus, are alternatives for long-term topical therapies. They are associated with milder and more manageable adverse effects, as they do not interfere with collagen synthesis, so the risk of skin atrophy is significantly lower compared to corticosteroids.32 However, they can cause pruritus and burning at the application site.
Although the indication for the treatment of psoriasis is not included in the package leaflet for TCIs, some studies have shown benefits. A study by Bissonnette et al. showed a satisfactory response and tolerability in a group of 12 men with genital psoriasis who used tacrolimus 0.1% ointment for 8 weeks.33 A study of 10 patients with facial and genital psoriasis showed that tacrolimus 0.1% ointment improved the symptoms of genital psoriasis after 12 weeks of use.34
Topical Vitamin D analogs, such as calcitriol and calcipotriol, are another class of drugs that can be used for a long time in genital and inverted psoriasis. In general, studies show that both calcitriol and calcipotriol are safe, but less effective than corticosteroids or TCI.35 A randomized direct comparison study between calcitriol 3 μg/g ointment and calcipotriol 50 μg/g ointment, both applied twice a day, showed that calcitriol was not only more effective, but also better tolerated in the treatment of inverted psoriasis.36
In general, phototherapy is not indicated for the treatment of genital psoriasis due to the increased risk of skin cancer in this area. A prospective study of 892 men with psoriasis exposed for a long time to psoralens and ultraviolet A (PUVA) radiation had an increased risk of tumors in the penis and scrotum, particularly squamous cell carcinoma. Furthermore, even after controlling for levels of exposure to PUVA, high levels of exposure to ultraviolet B radiation were also associated with an increased risk of genital cancer.37
Up to now, there have been no large clinical trials evaluating the efficacy and safety of traditional oral systemic therapies for genital psoriasis. One study demonstrated successful treatment with methotrexate, but a second described only a partial response to the drug.12,20 In addition, dapsone was used with a satisfactory response in two cases of pustular psoriasis affecting the skin of the penis.38,39 On the other hand, a randomized, placebo-controlled study showed that apremilast, an oral phosphodiesterase-4 inhibitor, improved the quality of life of patients with psoriasis involving limited and spatial areas, including the genitals.40 More specifically, another recent study evaluated the response to apremilast in patients with genital psoriasis, which also showed benefits.41
At present, the biologic agent with the specific indication for the treatment of genital psoriasis is ixekizumab, which is a high-affinity monoclonal antibody against interleukin (IL)-17A. Several studies have shown significant improvement in lesion appearance, pruritus, sexual health, and quality of life in patients with resistant genital psoriasis treated with ixekizumab.42–45 In addition, a Phase III, randomized, placebo-controlled clinical study demonstrated long-term efficacy and safety up to week 52 of treatment with ixekizumab.44 Patients received subcutaneous injections of 80 mg of ixekizumab (n = 74) or placebo (n = 74) every 2 weeks after an initial dose of 160 mg at week 0 until week 12; after which the study entered an open phase in which all patients received 80 mg every 4 weeks until week 52. As a result, in the initial phase of the study, 73% of the patients who received the drug achieved total or almost total improvement. Similarly, 79% of the patients who were initially in the placebo group achieved similar results at the end of week 52.
In addition to clinical trials, a real-life study involving 1978 patients with moderate to severe psoriasis, of whom around 25% had genital involvement, showed that in this subgroup of patients the IL-17A inhibitor biologics (ixekizumab and secukinumab) were significantly more effective than the other biologics agents used by the patients in the study (guselkumab, risankizumab, ustekinumab and adalimumab).46 When compared individually with ixekizumab, ustekinumab, and guselkumab were the least effective of the biologics agents used.
Similarly, in a real-life study of 255 patients with psoriasis treated with adalimumab, etanercept, or ustekinumab, genital psoriasis was associated with complete resolution of the condition (PASI100) when patients were treated with adalimumab.47 In this context, Orsini et al. showed satisfactory results in a real-life scenario in which patients with psoriasis were treated with risankizumab. Of a total of 202 patients, 72 had genital involvement. At the end of weeks 16, 28, and 52 of risankizumab use, 85%, 93% and 100% showed total or almost total improvement, respectively.48
Finally, the Italian GULLIVER study, a 12-week interim analysis, evaluated the efficacy and safety of guselkumab, a fully human monoclonal antibody targeting the p19 subunit of IL-23, in the treatment of genital and facial psoriasis. With 351 patients included, 204 of whom had genital psoriasis, it was observed that 76.5% of patients achieved an static physician’s global assessment score of 0 (clean) or 1 (almost clean) in the genital area after 12 weeks of treatment. As well as a significant improvement in erythema, thickness, and scaling scores in genital lesions, guselkumab also demonstrated a favorable safety profile, with only two mild and transient treatment-related adverse events. These results suggest that the IL-23 inhibitor is an effective and safe therapeutic option for patients with genital psoriasis.49,50 The management of genital psoriasis can be summarized in figure 3.
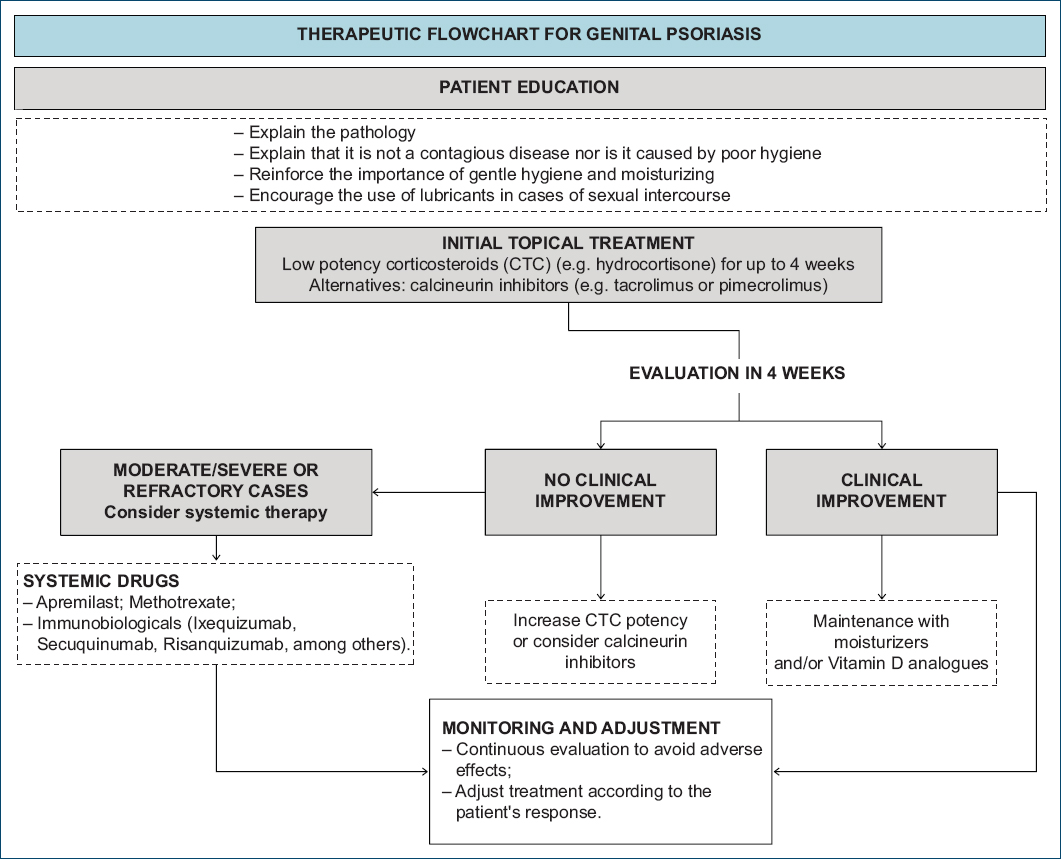
Figure 3. Therapeutic flowchart for genital psoriasis.
Conclusion
Genital psoriasis is a chronic and recurrent inflammatory disease, with a possibly underestimated prevalence, which significantly impacts patients’ physical, emotional, and sexual health. Its treatment involves considerable challenges; however, traditional therapies such as low-potency corticosteroids may be used as an initial approach. In addition, calcineurin inhibitors and Vitamin D analogues are alternatives for long-term topical therapies, due to their safety profile. More recent studies involving biologic therapies, particularly IL-17A and IL-23 inhibitors, have shown promising results in the management of refractory genital psoriasis, demonstrating improvements in both clinical outcomes and quality of life.
Funding
None.
Conflicts of interest
None.
Ethical considerations
Protection of human subjects and animals. The authors declare that no experiments on humans or animals were performed for this research.
Confidentiality, informed consent, and ethical approval. The authors have followed their institution’s confidentiality protocols, obtained informed consent from all patients, and secured approval from the Ethics Committee. SAGER guidelines have been followed as applicable to the nature of the study.
Declaration on the use of artificial intelligence. The authors declare that no generative artificial intelligence was used in the writing or creation of the content of this manuscript.
