Introduction
Herpes simplex virus (HSV) infection commonly involves skin, mucous membranes, eye, and central nervous system. Out of the two serologic types of HSV, HSV2 is more commonly associated with genital herpes. Lymphadenitis is a rare complication of HSV and can occur as a part of a systemic HSV involvement or associated with skin rash.1 Rarely, isolated lymphadenitis without any other evidence of HSV infection can also occur. Microscopic findings and correlation with serology becomes very important in these cases. Although histopathological features of HSV lymphadenitis are well documented, literature on cytomorphological features is scarce.2,3 We describe the cytology findings of HSV lymphadenitis in a young immunocompetent female with inguinal lymphadenopathy and vulvar lesions.
Case report
A 23-year-old woman presented with a swelling in the groin region for the past 3 weeks. It was gradually progressive, associated with dull ache and on and off fever. On examination, a firm, fixed, non-tender lymph node (LN) of 2 × 1.5 cm was palpable in the inguinal region along with an erythematous painful non-ulcerated lesion on the labia majora (Fig. 1). There were no other vulvar or vaginal lesions. She had had no treatment before and her past medical history revealed only an episode of Bell’s palsy 8 months beforehand that resolved in 4 months. The patient was sexually active and in a monogamous relationship for the past 3 years.

Figure 1. Clinical picture showing inguinal lymph node measuring 2 × 1.5 cm.
Fine-needle aspiration (FNA) from the inguinal LN yielded purulent material. FNA smears showed an inflammatory background consisting of neutrophils, many histiocytes, and multinucleated giant cells and occasional mononuclear cells with ground glass nuclei and occasional intranuclear inclusion (Figs. 2 and 3). A cell block was also made and immunohistochemistry (IHC) with HSV1 and 2 was performed. The cells showed nuclear immunoreactivity with HSV2. Serology with HSV also came positive (Fig. 4). Viral serology for human immunodeficiency virus, hepatitis B virus, and hepatitis C virus was also done and came to be negative. Thus, a final diagnosis of HSV lymphadenitis was rendered. Complete blood count revealed normal findings. The patient received acyclovir for 10 days following which the swelling disappeared. At 6 months of follow-up, the patient is doing well and is free of recurrence.
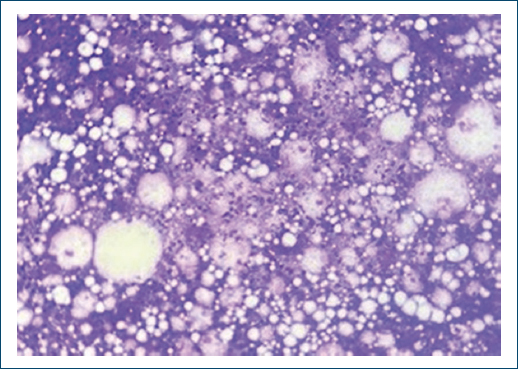
Figure 2. Fine-needle aspiration smear showing necroinflammatory background with neutrophils, histiocytes, binucleate histiocytes, and lymphocytes. Giemsa: ×200.
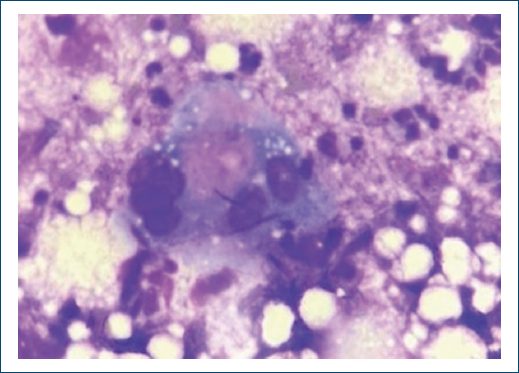
Figure 3. Fine-needle aspiration smear showing necroinflammatory background with multinucleated giant cell showing multinucleation, molding, and ground glass nuclei with occasional intra-nuclear inclusion. Giemsa: ×400.
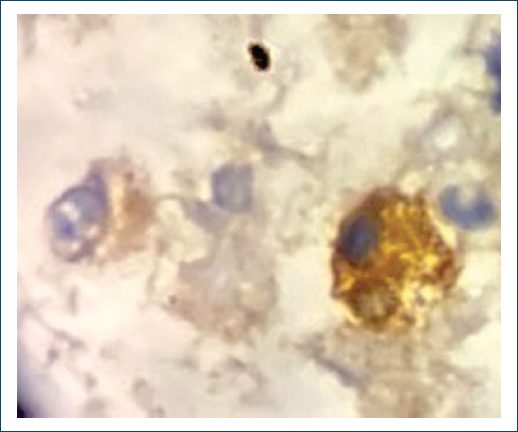
Figure 4. Nuclear positivity with herpes simplex virus 2 antigen ×1000.
Discussion
HSV has two serologic types: HSV1 and HSV2. Genital infection is more commonly seen with HSV2 and non-genital involvement with HSV1; however, overlap is seen.1 HSV is a deoxyribonucleic acid (DNA) virus with the ability to establish latent infection, which might get reactivated and disseminated in case of immunocompromised state. Isolated lymphadenopathy in HSV infection with or without associated mucocutaneous involvement is rarely seen, especially in immunocompetent host. Although HSV infection runs an indolent and self-limited course, HSV lymphadenitis needs to be diagnosed timely due to its well-documented association with hematologic malignancies. In a review of 27 cases of HSV lymphadenitis by Robertson et al.,4 11 out of 27 cases were immunocompetent while 16 had comorbidities that included lymphomas (10), leukemias (one acute myelocytic leukemia and one chronic myelocytic leukemia), steroid therapy (2), and immunodeficiency disorders (2). Out of these, HSV is more commonly associated with chronic lymphocytic leukemia. Inguinal LNs were most commonly involved followed by cervical. Cases of hematologic malignancies developing after their diagnosis of HSV lymphadenitis have also been reported.5 Thus, diagnosis of HSV lymphadenitis also warrants a hematologic work up as well as follow-up of the patient.
Various histomorphological features observed in HSV lymphadenitis include prominent paracortical expansion, follicular hyperplasia, dilated sinusoids filled with histiocytes, lymphocytes, and immunoblasts and monocytoid B-cell hyperplasia and often variable necrotic areas with neutrophils, karyorrhexic nuclear material, and smudged eosinophilic cellular ghosts of necrotic cells.6 Cells with viral cytopathic effects such as “ground-glass” nuclei, viral-like inclusions, and multinucleated giant cells can also be observed as well as necrotizing granulomatous inflammation.7 However, many of these features overlap with those seen in viral lymphadenopathies such as cytomegalovirus and Epstein-Barr virus. If HSV is associated with necrotizing granulomatous inflammation, tuberculosis, fungi, atypical mycobacteria, Yersinia, lymphogranuloma venereum, and cat-scratch disease need to be ruled out. Necrosis with karyorrhectic bodies along with prominence of phagocytic mononuclear cells also gives rise to the differential of Kikuchi’s disease. Thus, demonstration of HSV by serological studies, IHC or DNA hybridization, is essential in definitive diagnosis. Cytopathological findings include balloon like nuclear degeneration, margination of nuclear chromatin along the nuclear membranes, ground glass nuclei, intranuclear eosinophilic inclusion bodies, and cells with bi, tri, and multinucleation with nuclei lined in private soldier such as pattern and mosaic arrangement.2,3 The background is necrotic and inflammatory. In the present case, fine-needle aspiration cytology findings included necrosis, multinucleated giant cells, nuclear margination, and ground glass nuclei.
HSV leads an indolent course and is a self-limited disease. Treatment with acyclovir is well tolerated. HSV lymphadenitis is relatively rare, even in the setting of generalized HSV infection. HSV should be considered in the differential diagnosis of inguinal lymphadenopathy, especially when the LN is tender. HSV lymphadenitis should prompt a complete hematologic and immunologic work up of the patient.
Funding
None.
Conflicts of interest
None.
Ethical considerations
Protection of human subjects and animals. The authors declare that no experiments on humans or animals were performed for this research.
Confidentiality, informed consent, and ethical approval. The authors have followed their institution’s confidentiality protocols, obtained informed consent from all patients, and secured approval from the Ethics Committee. SAGER guidelines have been followed as applicable to the nature of the study.
Declaration on the use of artificial intelligence. The authors declare that no generative artificial intelligence was used in the writing or creation of the content of this manuscript.
