Introduction
Elastosis perforans serpiginosa (EPS) is a rare perforating dermatosis characterized by transepidermal elimination of altered elastic fibers from the dermis1. It belongs to the primary perforating disorders, where degenerated elastic tissue is extruded through epidermal channels, forming distinctive lesions2. EPS typically presents in childhood or early adulthood with a male predominance and an estimated prevalence of < 1 in 100,0003. Clinically, it manifests as asymptomatic, hyperkeratotic papules arranged in arcuate, serpiginous, or annular patterns, commonly on the neck, face, or upper extremities4. Lesions are often self-limiting but may persist or recur.
EPS is classified into idiopathic (50-70% of cases), reactive (associated with connective tissue disorders such as pseudoxanthoma elasticum, Ehlers–Danlos syndrome, or Down syndrome), and drug-induced (commonly linked to long-term penicillamine therapy)5–7.
Associated comorbidities include cardiovascular anomalies, renal diseases, or intellectual disabilities in syndromic cases8. Histopathologically, EPS shows acanthosis, hyperkeratosis, and transepidermal channels containing basophilic debris and fragmented elastic fibers, confirmed by Verhoeff-van Gieson (VVG) staining9. The etiology involves altered elastin metabolism, possibly due to genetic mutations or external triggers affecting dermal fibroblasts3. Diagnosis is clinicopathologic, as clinical mimics include granuloma annulare, porokeratosis, or reactive perforating collagenosis10. Treatment is challenging, with topical retinoids, cryotherapy, or laser ablation used anecdotally11,12. This case report describes an atypical presentation of idiopathic EPS in a middle-aged adult, highlighting diagnostic challenges and therapeutic success.
Case report
A 38-year-old male presented to the dermatology outpatient department with multiple solid lesions on the neck for 6 months. The lesions were insidious in onset, gradually increasing in number, painless but intensely pruritic, impacting daily activities. He denied preceding trauma, drug intake (including penicillamine), family history of similar lesions, or systemic symptoms such as joint pains or cardiovascular issues. No comorbidities, including connective tissue disorders or genetic syndromes, were reported. Examination revealed multiple non-tender, arcuate plaques bilaterally over the nape of the neck, surrounded by 2-3 mm keratotic papules in a serpiginous pattern, without scaling, ulceration, or erythema (Figs. 1 A and B). No lesions were noted elsewhere. Differential diagnoses included granuloma annulare, annular elastolytic giant cell granuloma, and porokeratosis, but the morphology suggested a perforating disorder.
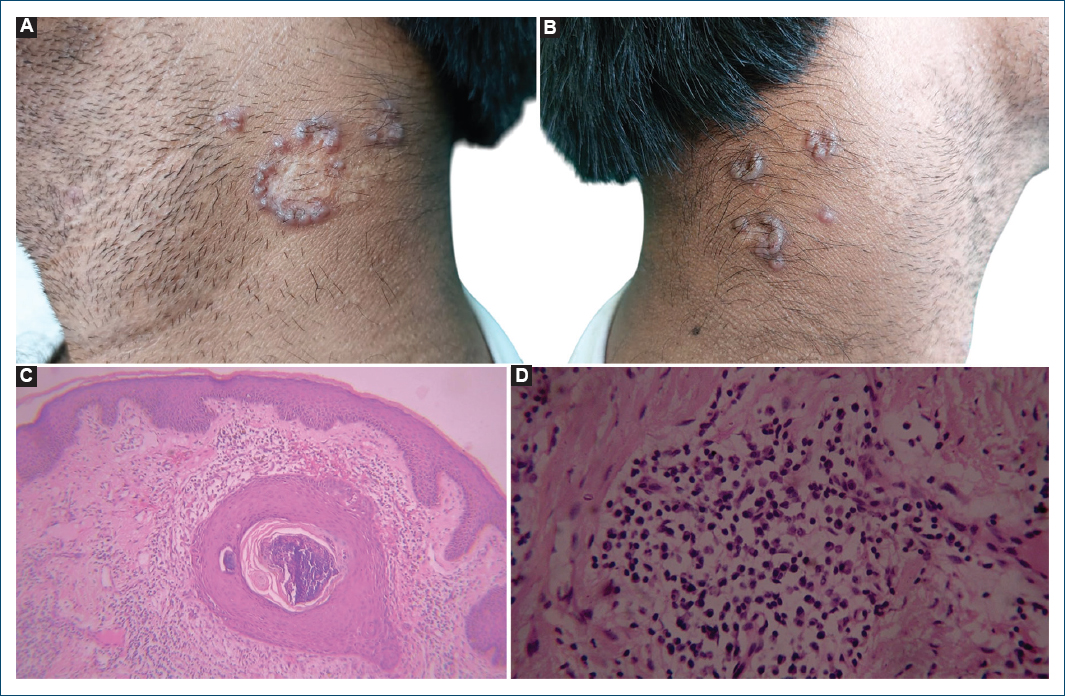
Figure 1. Clinical and histopathological images. A and B: multiple arcuate plaques bilaterally over the nape of the neck, surrounded by 2-3 mm keratotic papules in a serpiginous pattern. C: ×10 magnification showing acanthosis, hyperkeratosis and transepidermal channels containing basophilic debris and fragmented elastic fibers. D: ×40 magnification showing mild lymphocytic and plasma cell infiltrates in dermis.
Laboratory investigations, including complete blood count and renal function tests, were normal. A punch biopsy from a lesion showed irregular acanthosis with elongated rete ridges forming narrow channels containing basophilic debris and thick, twisted elastic fibers (Fig. 1C). The dermis had mild lymphocytic and plasma cell infiltrates (Fig. 1D). Hematoxylin and eosin staining confirmed these findings, and VVG staining highlighted fragmented elastic fibers within the channels, consistent with EPS9. No collagen perforation or foreign material was seen. Idiopathic EPS was diagnosed based on clinical and histopathological correlation.
Topical 0.05% tretinoin cream was applied nightly. Pruritus improved within 2 weeks, and lesions resolved completely after 3 months, with no scarring or recurrence at 6-month follow-up.
Discussion
This case is atypical due to its late onset, intense pruritus, and idiopathic nature without associated factors. EPS typically presents before the age of 20 years, with only 15% of cases occurring after 30, often in reactive or drug-induced forms3. A systematic review of 68 EPS cases noted late-onset cases are rare and usually linked to comorbidities3. The intense pruritus here contrasts with the typically asymptomatic or mildly itchy EPS; pruritus is more common in acquired perforating dermatoses such as those associated with diabetes or renal failure, absent in this patient2,4. The dermal lymphocytic and plasma cell infiltrates suggest a heightened inflammatory response, though not typical for EPS9.
The absence of genetic, drug-related, or systemic associations marks this as a rare idiopathic variant. Approximately 25-40% of EPS cases relate to genetic disorders such as Down syndrome, where elastin synthesis may be disrupted8,13. Drug-induced EPS, comprising 20-30% of cases, is strongly associated with penicillamine, which alters elastin cross-linking5,6,14. Reactive EPS may occur with pseudoxanthoma elasticum or scabies, triggering elastic fiber degradation7,10. This patient’s lack of such factors suggests a sporadic elastin gene mutation or unidentified environmental trigger5.
Histopathology was crucial, showing classic EPS features: transepidermal channels with elastic debris, confirmed by VVG staining9. This distinguishes EPS from reactive perforating collagenosis, which involves collagen2. Topical tretinoin led to complete resolution, consistent with its role in promoting epidermal turnover and elastic fiber clearance11,12. Alternatives such as cryotherapy or CO2 laser are less effective, and systemic isotretinoin is reserved for refractory cases4,11. In drug-induced EPS, discontinuing the offending agent is critical, though lesions may persist6. Rare paraneoplastic associations with malignancies like multiple myeloma necessitate systemic evaluation in atypical adult-onset cases7.
This case underscores the diagnostic challenge of atypical EPS, where biopsy is essential. Future research should explore genetic profiling to clarify idiopathic cases and optimize therapies.
Conclusion
This late-onset, pruritic, idiopathic EPS case without comorbidities highlights the variability of this rare dermatosis. Histopathologic confirmation and topical tretinoin therapy led to resolution, emphasizing conservative management. Clinicians should consider EPS in adults with serpiginous neck lesions, even without classical associations, to avoid misdiagnosis. This report adds to the literature on atypical EPS, advocating for increased awareness in dermatologic practice.
Funding
None.
Conflicts of interest
None.
Ethical considerations
Protection of humans and animals. The authors declare that no experiments involving humans or animals were conducted for this research.
Confidentiality, informed consent, and ethical approval. The authors have followed their institution’s confidentiality protocols, obtained informed consent from patients, and received approval from the ethics committee. The SAGER guidelines were followed according to the nature of the study.
Declaration on the use of artificial intelligence (AI). The authors declare that no generative artificial intelligence was used in the writing of this manuscript.
