Introduction
The Varicella-Zoster Virus (VZV), which causes chickenpox, belongs to the Herpesviridae family.1 A hallmark of these viruses is their ability to establish latency, following primary infection or vaccination.2 VZV persists in a dormant state within sensory neurons; declining VZV-specific cell-mediated immunity can trigger reactivation, resulting in herpes zoster (HZ).3 The latter typically presents as a painful, unilateral dermatomal vesicular rash.4 HZ is common in older adults, with an incidence of 3-5/1,000 person-years, rising sharply after age 50, and a recurrence rate of approximately 5%.5 In contrast, HZ remains an uncommon cause of rash in children.6 While traditionally associated with immunocompromised pediatric patients, recent reports have documented an increasing number of cases in otherwise healthy, immunocompetent children.7 This retrospective case series aimed to describe the clinical characteristics, associated conditions, treatment approaches, and complications of HZ in children at our center, to promote early diagnosis and minimize complications.
Method
A retrospective observational study was conducted at the Dermatology Department of Hassan II University Hospital, Faculty of Medicine and Pharmacy, Sidi Mohamed Ben Abdellah University, Fez, Morocco. The study period extended from February 01, 2016, to April 30, 2025. Consecutive cases of pediatric HZ were identified by searching the hospital’s electronic database using the keywords “herpes zoster” or “zona” in the diagnosis field. All children clinically diagnosed with HZ by a certified dermatologist were considered for inclusion. The clinical diagnosis was established based on a characteristic unilateral, dermatomal vesicular eruption, frequently accompanied by pain or dysesthesia; no PCR testing was performed or required, as the presentation was typical in these pediatric cases. Inclusion criteria were: (1) a clinical diagnosis of HZ and (2) age ≤ 18 years at the time of diagnosis. Exclusion criteria included patients aged > 18 years or those with incomplete medical records regarding the studied variables (2 patients were excluded due to missing key data, such as follow-up until resolution or treatment details). Patient confidentiality was strictly maintained by anonymizing all personal identifiers during data entry. Written informed consent for the use of clinical photographs was obtained from parents or legal guardians. Relevant data were extracted from patient files using a standardized, pre-tested data collection form. Collected variables included: demographic characteristics (age, sex), clinical features (involved dermatome, rash characteristics), medical history (previous chickenpox, varicella vaccination status, underlying immunosuppressive conditions), and treatment details (antiviral therapy, analgesics).
Results
A total of 20 cases of HZ were managed in our department over a 9-year period. Sixty-five percent of patients (n = 13) were male, and 35% (n = 7) were female (Fig. 1), yielding a male-to-female ratio of 1.86. The mean age was 7.13 ± 3.77 years, with a range from 11 months to 14 years. A documented history of varicella was present in 7 patients (35%). In 10 cases, there was no history of varicella, or the families could not recall an episode. Two children had been exposed to the VZV in utero, and one patient had a history of suspected close contact with varicella. Three patients had an underlying neoplastic disease and were receiving immunosuppressive chemotherapy at the onset of HZ. None of the patients had received the varicella vaccine. Pruritus was the most common symptom, reported by 10 patients (50%). Pain and burning sensations were present in 4 patients (20%), while 6 patients experienced a combination of pain, pruritus, and fever. The thoracic dermatomes were the most frequently involved (55% of cases) (Fig. 2), followed by trigeminal involvement (30%) (Fig. 3). Among the latter, four patients developed ocular complications. Cervical and lumbosacral dermatomes accounted for 10% and 5% of cases, respectively (Fig. 4). Oral mucosal involvement was observed in only one patient, limited to the right hard palate in a case of trigeminal (V2) HZ (Fig. 5). One 9-year-old child presented with involvement of the right external ear and cervical dermatomes but showed no clinical signs of 7th or 8th cranial nerve dysfunction. Identified predisposing factors included malignancy in 15% of patients (2 cases of leukemia and 1 of medulloblastoma), asthma in 1 patient, and significant stress reported in 4 patients. Regarding acute complications, bacterial superinfection was the most common (30%), followed by ocular involvement manifesting as zoster keratitis in 4 patients (20%) and stage 1 orbital cellulitis (preseptal) (per Chandler’s classification) in 2 patients (10%). No neurological complications were recorded. All cases were diagnosed clinically based on detailed history and typical physical findings. Laboratory tests were unremarkable except for mild leukocytosis in three patients and mild anemia in one. Twelve patients (60%) received oral valacyclovir (80 mg/kg/day divided every 6 h), seven (35%) received intravenous acyclovir (20 mg/kg/day divided every 8 h), and one (5%) received symptomatic treatment only. All treated patients completed a 7- to 10-day course. The disease was self-limiting and resolved within two weeks in all but one case. One patient was left with a dyschromic macular patch and erythematous hypertrophic scarring (Fig. 6), which was subsequently managed with topical corticosteroids. Post-herpetic neuralgia was not observed in any patient during follow-up.
Figure 1. Out of 20 cases, 13 were males, 7 were females.

Figure 2. Intercostal shingles in an 11-year-old female child.

Figure 3. Ophthalmic shingles in a 10 year-old male child.
Figure 4. Site of involvement of herpes zoster.
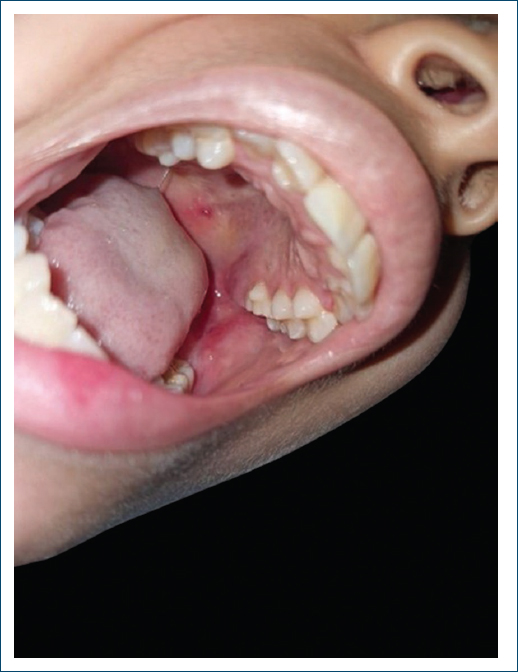
Figure 5. Oral mucosal involvement in a child with herpes zoster affecting the trigeminal dermatome.

Figure 6. Dyschromic macular patches and erythematous hypertrophic scarring in a 9-year-old boy, 6 months after resolution of herpes zoster involving the right cervical and trigeminal dermatomes.
Discussion
HZ, from the Greek “zoster” meaning belt or girdle; also called shingles from the Latin “cingulum”,8 has a generally low incidence in the pediatric population, with an estimated rate of 0.74 cases/1000 person-years, which is 4-7 times lower than in adults.9 The incidence progressively increases with age, from 0.4 cases/1000 person-years in children between the ages of 1 and 9 years to 1.06 in the group of children > 10 years.9 The primary risk factors for developing HZ in children are well-documented in the literature. These include maternal exposure to the VZV during pregnancy (with a risk of 0.8% for exposure at 13-24 weeks and 1.7% at 25-36 weeks).10 Another significant factor is the timing of the primary varicella infection; contracting chickenpox within the 1st year of life carries a substantially higher risk, with an incidence of 410/100,000 person-years and a mean interval to zoster of 3.8 years, compared to 45/100,000 person-years and a mean interval of 6.2 years for infection after the 1st year.10 Furthermore, immunocompromised states, such as malignancies, constitute a well-established risk factor, confer a 5-6 times higher risk due to cellular immunosuppression from the disease or its treatments (e.g., chemotherapy, radiotherapy).5,11 Conditions, such as asthma are associated with a two-fold increase in HZ risk.10 In our cohort, some of these factors were observed: malignancy (15%), reported significant stress (20%), and asthma (5%). In addition, 35% had a documented history of varicella, and two children had been exposed to VZV in utero. The absence of classic immunosuppression in most of our patients underscores that HZ can develop in immunocompetent children. The mean age in our study was 7.13 ± 3.77 years (range: 11 months-14 years), indicating a predominance in school-age children, with a male predominance, this aligns with a Turkish study of 60 pediatric HZ cases, which reported a mean age of 8 ± 4.93 years and a male predominance (37 boys vs. 23 girls).7 Diagnosis is primarily clinical, characterized by a painful, erythematous, maculopapular rash that rapidly progresses, within a single dermatome and without crossing the midline, to clear-fluid-filled vesicles, which subsequently become pustular and then crust over.12 Unlike in adults, where pain predominates, itching is the most common symptom in children, followed by pain, fever, and weakness.13 Our findings are consistent with pruritus reported in 50% of cases. Thoracic dermatomes are most frequently involved in children,7,8,14 a pattern reflected in our series (55% of cases), followed by trigeminal, cervical, and lumbosacral involvement. Although generally self-limiting, systemic antiviral therapy is indicated for immunodeficiency, disseminated disease, or ophthalmic involvement (especially with nasociliary branch involvement.10 Treatment may also be considered for otherwise healthy children to prevent scarring, ocular complications, and acute pain.15 Early initiation (within 72 h of rash onset) for at least 7 days accelerates healing and reduces complications,8,12,16 as applied in our case series. Potential complications include secondary bacterial infection, ocular involvement, neurological sequelae, and scarring.4 In our series, acute complications occurred in 60% of patients, most commonly secondary bacterial superinfection (30%) and keratitis (20%, all with trigeminal involvement). No neurological complications or post-herpetic neuralgia were observed, consistent with other pediatric studies.7,17 One patient developed permanent dyschromic macules and hypertrophic scarring.
Conclusion
HZ is an uncommon, generally self-limited condition in children, typically characterized more by pruritus than by pain, and carries a minimal risk of post-herpetic neuralgia. Nevertheless, complications, such as bacterial superinfection and ocular involvement necessitate close monitoring. Importantly, our study revealed that most affected children were immunocompetent, highlighting that HZ can occur without classic risk factors or underlying immunodeficiency. Consequently, HZ should be considered in any child presenting with a dermatomal vesicular rash. Early recognition and prompt antiviral therapy remain the cornerstone to prevent morbidity.
Funding
None.
Conflicts of interest
None.
Ethical considerations
Protection of human subjects and animals. The authors declare that no experiments on humans or animals were performed for this research.
Confidentiality, informed consent, and ethical approval. The authors have followed their institution’s confidentiality protocols, obtained informed consent from all patients, and secured approval from the Ethics Committee. SAGER guidelines have been followed as applicable to the nature of the study.
Declaration on the use of artificial intelligence. The authors declare that no generative artificial intelligence was used in the writing or creation of the content of this manuscript.
