Introduction
Port-wine stains (PWS), also known as nevus flammeus represents a dermal capillary hamartomatous malformation and are the most common benign congenital capillary malformation. Its prevalence is reported to be 0.3-1%, with females being affected twice as often as males.1 It clinically presents as a well-defined unilateral, bilateral, or centrally placed pink to red patch that is present at the time of birth. It persists throughout life and progressively darkens in later life, and can potentially form nodules or hypertrophic plaques in adulthood. It can be localized in any part of the body but has a predilection for the head and neck.2
Cases are usually sporadic, but in 10% of the cases, familial incidence and an autosomal dominant inheritance have been described.3 PWS can be part of syndromes such as Sturge-Webe syndrome, a nonfamilial congenital disease with ocular and intracranial complications or neurological deficits, or Klippel-Trenaunay Syndrome with limb overgrowth.
Acquired port-wine stains are rarely observed, often reported in adolescents or adults, usually following trauma. They are clinically and histopathologically indistinguishable from congenital capillary malformation.
Dermoscopy has emerged as a valuable tool for evaluating vascular morphology non-invasively, contributing both to the diagnosis and treatment planning. Although dermoscopy has been used in the evaluation of PWS, there are limited data on its application in Indian populations. This case series of 17 patients from eastern India highlights distinct dermoscopic features in the skin of higher phototypes, with possible implications for diagnosis and lesion monitoring. In addition, we explore correlations with lesion site and morphology, contributing novel insights to the existing literature.
Methods
A prospective observational analysis was conducted at dermatology outpatient department of a tertiary care center in eastern India over 12 months (March 2024-March 2025). Seventeen patients with clinically diagnosed PWS were included in the study after giving their informed consent or their guardian’s consent.
Clinical data, including age, sex, lesion site, and brief history, were noted. Each patient underwent a clinical examination followed by dermoscopic evaluation using non-polarized DermLite DL5 dermoscope. Images were recorded using an iPhone 15, focusing uniformly over central most region of the PWS. Vascular morphology, as well as other relevant dermoscopic findings, were recorded and correlated with lesional age and localization.
Results
Seventeen patients with PWS, 6 males and 11 females (male-to-female ratio 2:3), were analyzed in this series. Patients’ age ranged from 6 to 34 years (mean 17.6 ± 8.7 years). Within this group, 13 (76.47%) patients presented with PWS on the head-and-neck region (Fig. 1); two (11.76%) patients had involvement of the lower limb, and two (11.76%) patients the upper limb. Among these, one (5.88%) patient also had tongue involvement, and another had developed a 0.5 × 0.5 cm soft nodule over the PWS on the trunk at the age of 32 years (Fig. 2 and Table 1). All the lesions were present at birth, and all the patients were asymptomatic, with the sole complaint being a cosmetic concern.

Figure 1. Clinical image of port-wine stain over left aspect of face disturbed over nose, malar region and left zygomatic arch taken by iPhone 15.

Figure 2. Clinical image of nodule over background of port-wine stain over trunk taken by iPhone 15.
Table 1. Age distribution of patients, localization of port-wine stain, fitzpatrick skin type and dermoscopic findings
| Age group | Location | Fitzpatric skin type | Dermoscopic fingings | ||
|---|---|---|---|---|---|
| Background | Vessel morphology | ||||
| 5-10 (n = 4) | Face | V (n = 4) | Red-white background | Dots, globules, reticular arrangement | |
| 11-15 (n = 6) | Face | IV (n = 1), V (n = 5) | Red-white background | Dots, globules | |
| 16-20 (n = 3) | Face, dorsum of foot, tongue | IV (n = 1), V (n = 2) | Red-white background | Dots, globules, linear vessels | |
| 21-25 (n = 1) | Dorsum of foot | V (n = 1) | Brown background | Dots, globules | |
| 26-30 (n = 0) | – | – | – | – | |
| 31-35 (n = 3) | Trunk, upper limb | V (n = 3) | Brown background | Dots, globules, sauage vessels, nodule | |
Dermoscopic evaluation revealed a varied vascular morphology, with the most common finding being dots and globules observed in all patients (100%). In additon, linear vessels were present in 16 cases of PWS (94.11%) and sausage-shaped vessels in four (23.52 %) (Fig. 3). Two most observed non-vascular characteristics were white veil and reticulate hyperpigmentation, the latter being twice as common as the former, mostly seen in PWS involving the face. One patient (5.88%) had a globular nodule over a background of PWS (Fig. 4). With increasing age, findings progressed from red-white background with superficial vascular patterns, mainly dots and globules, to brown background along with emergence of sausage-shaped vessels and nodular changes in the higher age group. Table 1 summarizes the demographic data, location of PWS, skin type, and their dermoscopic findings.
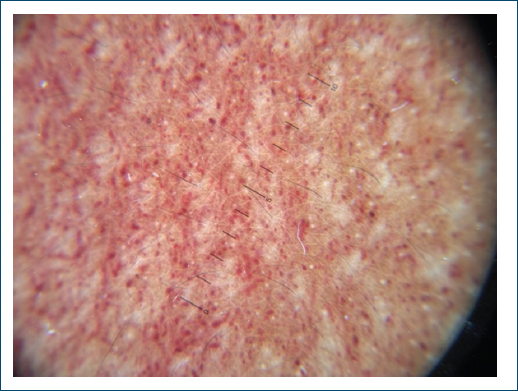
Figure 3. Dermoscopic image obtained using DermLite DL5 dermoscope at ×10 magnification depicting dots, globules, linear vessels and sausage vessels.
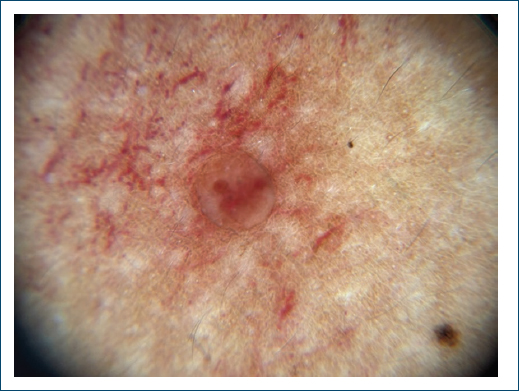
Figure 4. Dermoscopic image of nodule over background of port-wine stain at ×10 magnification visualized through DermLite DL5 dermoscope.
Discussion
Port-wine stains are congenital vascular malformations characterized by ectatic dermal blood vessels that appear at birth and persist throughout life, often progressing in color and surface morphology over time. The treatment includes vascular targeting lasers such as intense pulsed light (IPL), pulsed dye laser (PDL), and recently also photodynamic therapy. Dermoscopy is a useful tool in evaluating various dermatological conditions involving blood vessel abnormalities, and, in the case of PWS, it may contribute to predict therapy response.
The capillaroscopic pattern of PWS can be divided into Type I (dots or globules which represent vertical capillaries located in the papillary dermis), Type II (linear vessels and reticular vessels representing horizontal capillaries in the reticular dermis),4 and Type III (mixed vessels that exhibit combined features of both Type I and Type II capillaroscopic pattern.5 Our series offers an insight into dermatological patterns of PWS. The presence of dots and globules was the most common finding, more prevalent in the younger age group, aligning with the findings of Ngoc et al.6 Linear vessel pattern was the second most common vascular morphology in our study, also in agreement with Ngoc et al., while Huang et al. found it to be the most common pattern. Mixed vessel pattern was seen in lower frequency and in the older age group, mirroring the associations reported by Huang et al. with chronicity.5 Looped vessels or sausage-shaped vessel and complications such as nodule formation were reported in thicker and more hypertrophic PWS.5 Minkis et al. reported that approximately 65% of PWS become hypertrophic or nodular by the fifth decade of life, indicating PWS do not involute spontaneously, but rather tend to evolve over time.7 Table 2 compares the various dermoscopic findings seen in our series with those of Huang et al.4 and Ngoc et al.6
Table 2. Comparison of our study with Huang et al.4 and Ngoc et al.6
| Dermoscopic feature | n = 17 (%) | Huang et al. n = 264 (%) | Ngoc et al. n = 148 (%) |
|---|---|---|---|
| Dots and globules | 17 (100) | 9.10 | 76.40 |
| Linear vessels | 16 (94.11) | 42.00 | 68.90 |
| Whitish veil | 7 (41.17) | 38.30 | 29.10 |
| Reticular hyperpigmentation | 15 (88.23) | – | – |
| Mixed vessels | 4 (26.66) | 19 (7.2) | 47 (31.8) |
The relevance of these dermoscopic vascular patterns extends beyond morphological classification and has implications for response to laser therapy. Prior histopathological and laser response studies have demonstrated that vessel depth and diameter are critical determinants of laser efficacy8. Shirakawa et al. emphasized that superficial vessels show a better response to laser therapy, while treatment efficacy diminishes as vessels become deeper. Vessel diameter also plays a key role: larger, superficial vessels respond more favorably to laser treatment compared with smaller diameter vessels located deeper in the dermis. These findings suggest that dermoscopic patterns dominated by dots and globules representing superficial papillary dermal vessels are more amenable to PDL or IPL therapy9. In addition, laser therapy for PWS may be less effective in individuals with higher Fitzpatrick skin types due to higher epidermal melanin, which limits energy penetration, thereby influencing treatment outcomes despite having favorable dermoscopic vascular patterns.10
Bhagwat et al. studied the utility of dermoscopy in pediatric vascular anomalies, in which they recruited 61 patients below 18 years of age. Out of 61, 8 presented with PWS, where the dermoscopic findings were classified as dots, globules, and a broken network of thick and/or thin vessels. They emphasized the reticular arrangement pattern, which was not visualized in our study due to the lesser magnification as compared to the video dermoscopy used in their study.11
Limitations of our study included the small number of patients studied, which did not allow for a good correlation of dermoscopic parameters with age or localization of the lesion. Furthermore, as treatment was not evaluated, we could not confirm the utility of dermscopy as a predictor of treatment response.
Although various case series on dermoscopy of PWS exist, findings in Indian skin have not been evaluated before. Our case series highlights the utility of dermoscopy in the correct diagnosis. Dots, globules, and linear vessels are more favorable indicators occurring in the younger age group, while mixed patterns occur over time.
Our case series highlights the utility of dermoscopy in diagnosis but also as a potential prognostic adjunct in PWS. Dots, globules, and linear vessels are more favorable indicators reflecting their association with earlier disease stage and their known responsiveness to treatment, while mixed patterns occur over time. Dermoscopic identification of superficial vascular patterns may help anticipate treatment response and guide patient counseling.
Funding
None.
Conflicts of interest
None.
Ethical considerations
Protection of humans and animals. The authors declare that no experiments involving humans or animals were conducted for this research.
Confidentiality, informed consent, and ethical approval. The authors have followed their institution’s confidentiality protocols, obtained informed consent from patients, and received approval from the Ethics Committee. The SAGER guidelines were followed according to the nature of the study.
Declaration on the use of artificial intelligence. The authors declare that artificial intelligence was used in the writing of this manuscript for the translation of the abstract section from English to Portuguese.
